Etiology
The first trimester is crucial for the genesis of limb production. Congenital limb deficiency occurs as a result of failure of formation of part or all of the limb bud. The mesodermal formation of the limb occurs at 26 days gestation and continues with differentiation until 8 weeks gestation.
The various limb segments develop in a proximal-to-distal order so that the arm and forearm appear before the hand, and the thigh and leg before the foot (6). Limb development is a complex process that involves orchestration of a number of genes; some are well known and studied, and account for various syndromes and abnormalities (7). A relatively small set of genes and gene families appear to control the early stages of limb development. More than 80% of heritable limb deficiencies are associated with anomalies outside the musculoskeletal system (7).Upper limb deficiencies are more commonly associated with other anomalies, particularly craniofacial, cardiac, and hematological disorders; this is due to the chronology of development in the first trimester (8). Bilateral deficiencies are more common with craniofacial abnormalities, whereas left-right asymmetry of organogenesis is more commonly associated with unilateral and left axial deficiency (9,10). Vascular pathology is not inherited, so the risk of recurrence is small (7). Conditions with implied vascular disruption include Adams-Oliver syndrome, gastroschisis, Klippel-Feil syndrome, Moebius syndrome, Poland syndrome/sequence, and terminal transverse limb deficiency (11-13). Two key features of Moebius are demonstrated in Figure 13.1: craniofacial anomalies and upper limb deformity.
Other factors that put a child at risk for limb deficiency include maternal diabetes, including gestational diabetes (14,15). Although alcohol, heroin, and cocaine have not been found to be related to limb deficiency, all maternal ingestions
A
B
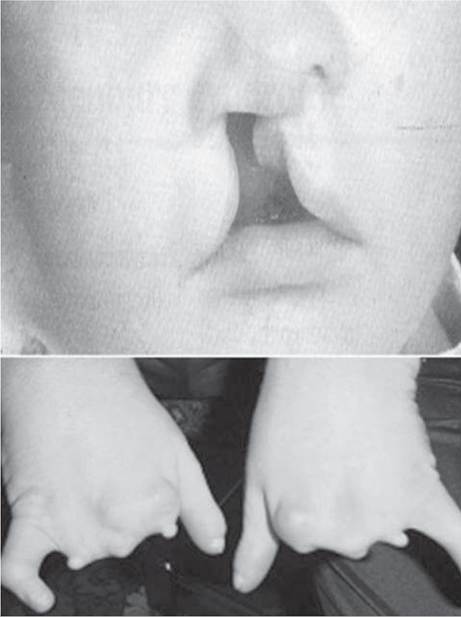
Figure 13.1 Two key components of clinical presentation in Moebius syndrome.
Craniofacial (A) and upper-limb (B) deformities.and first-trimester abnormalities should be documented (16,17). Smoking increases the risk of digit anomalies (18). Thalidomide historically presents a clear association with limb reductions (19). Recent case reports implicate valproic acid and calcium channel blockers (20,21). Maternal occupation may play a role, with exposure to chemicals, as in the agricultural setting (22). Uterine abnormalities have been reported in several cases of limb deficiencies, theoretically due to compression of the fetus (6). In addition, disturbances to the uterine environment, such as chorionic villi sampling, are implicated in deficiencies (23). Amniotic band syndrome is associated with fibrous bands that may constrict the limbs (24,25). Radiological findings of amniotic band are illustrated in Figure 13.2. Prenatal vitamins reduce the risk of limb deficiencies (26).
Postnatal problems, such as gangrene from vascular emboli and neonatal injury from vascular compromise secondary to umbilical catheters, may necessitate immediate amputation (27-29). Although the causes may be different from congenital disorders, the clinical issues for the child and the rehabilitation team are more similar to congenital disorders than acquired disorders.

Figure 13.2 X-ray of hands affected by amniotic band syndrome.
More on the topic Etiology:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Control of BTB in Ethiopia