EXERCISE IN PEDIATRICS: PSYCHOSOCIAL IMPACT
Regular physical activity in early childhood through adolescence fosters not only improvements in physical health, but also psychosocial health and development (29,30). The amount and quality of physical activity has significantly declined over the past several decades and even able-bodied (AB) children are no longer meeting the recommended guideline of one hour or more of moderate-intensity physical activity on five or more days a week (31).
In disabled children, the amount of physical activity is even more restricted due to a variety of factors, including the underlying disability, physical barriers, and availability of resources (32). Sit et al. noted that the amount of time spent by children in moderate physical activity at school during PE and recess was lowest for children with a physical disability, at 8.9%, and highest for children with a hearing impairment, at 16.6% of recommended weekly minutes (33). Studies involving AB children have demonstrated that providing game equipment and encouragement from teachers can significantly increase moderate activity levels during recess time (34). Deviterne et al reported that providing participant-specific written and illustrated instruction concerning sporting activities such as archery to adolescents with motor handicaps improves their skill performance to a level similar to an AB adolescent at the end of the learning session that can foster increased self-esteem (35).Many studies have demonstrated increased social isolation with fewer friendships among disabled children and adolescents. The Ontario Child Health Study revealed that children with a chronic disability had
5.4 times greater risk of being socially isolated and
3.4 times greater risk of psychiatric problems (36). Mainstreaming seems to have a positive impact, although concerns regarding AB peer rejection are still pervasive (37).
Children in integrated PE programs were more likely to view their disabled peers as “fun” and “interesting” compared to children who were not integrated (38). One study of teacher expectations in mainstreamed PE classes revealed significantly lower expectations for the disabled student's social relations with peers (39). The attitude toward mainstreamed PE among high school students was significantly more positive in the AB group as opposed to the disabled population (40). Disabled children often view their lack of physical competence and secondly the status among their peers as the major barriers in social competence (41).In addition to regular physical activity, play is a major component of childhood and important in psychosocial development of children. In preschool children with developmental delay or mental retardation, they were more likely to play on their own or not participate in play compared to the typically developing peers. Placing them in an integrated playgroup increased peer interactions compared to a nonintegrated playgroup, but did not correct the discrepancy in sociometric measures (42). There have also been discrepancies noted in the type of play for children with developmental delays. These children are less likely to participate in imaginative or constructive play (ie, creating something using the play materials) and more likely to participate in functional (ie, simple repetitive tasks) and exploratory play (43). It has been suggested that play should be taught, and one study by DiCarlo demonstrated that a program that taught pretend play increased independent pretend toy play in 2-year-old children with disabilities (44).
Play for children with physical disabilities is also impaired. Children rely on technical aids such as bracing, walkers, wheelchairs, or adult assistants to access play areas and play equipment. Studies have shown that they are seldom invited to spontaneous playgroups and rarely take part in sporting activities unless the activity is geared toward children with disabilities (45).
In a study by Tamm and Prellwitz, preschool and schoolchildren in Sweden were surveyed about how they viewed children in a wheelchair. They were willing to include disabled children in their games, but saw barriers to participation in outdoor activities due to the inaccessibility of playgrounds and the effect of weather. They did not feel disabled children would be able to participate in activities like ice hockey, but could play dice games. They felt sedentary and indoor activities were more accessible. The children also felt that disabled children would have high self-esteem, although most literature has documented that disabled children have low self-esteem (46).In another study, children with motor disabilities were surveyed regarding how they perceived their technical aids in play situations. Younger children viewed their braces, crutches, walkers, or wheelchairs as an extension of themselves and helpful in play situations. Older children also saw the equipment as helpful, but a hindrance in their social life, as it made them different from their peers. Both older and younger children saw the environment as a significant barrier to play. Playgrounds often had fencing surrounding the area, sand, and equipment such as swings or slides that were not accessible without the assistance of an adult. The weather impacted accessibility due to difficulty maneuvering on ice or through snow. Children often took on an observational role on the playground or stayed inside. It was noted that the lack of accessibility sent the message that the DA children were not welcome and further isolated the DA group. As far as adult assistance, the younger children often incorporated the adult as a playmate. As children became older, they viewed their adult assistants as intrusive and a hindrance in social situations. Older children often chose to stay at home and be alone rather than going somewhere with an adult (45).
The research has highlighted many areas for improvement in accessibility for play and social interaction. Several articles detail ways to create accessible playgrounds, and these playgrounds are now becoming more prevalent in the community (Fig. 5.1). Playground surfaces can be covered with rubber, and ramps can be incorporated throughout the play structure to allow access by wheelchairs, walkers, and other assistive devices. Playground equipment can include wheelchair swings and seesaws that allow a wheelchair placement (47).
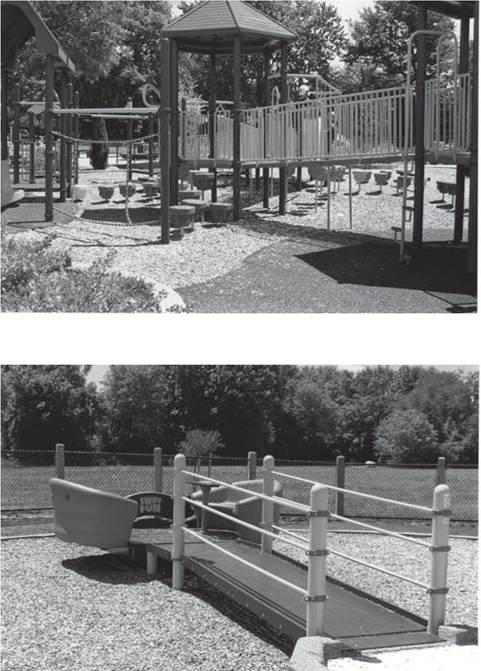
Figure 5.1 Playground equipment can be adapted to include children of all abilities, including pathways for wheelchair and walker access.