HEMORRHAGIC DISORDERS
The term Hemorrhagic disorders includes a group of heterogeneous congenital or acquired defects, all characterized by abnormal tendency to bleed, either spontaneously or after trauma.
Though frequently used interchangeably, the term bleeding disorders denotes platelet dysfunction, while coagulation disorders refer to abnormalities of clotting cascade.Etiologically hemorrhagic disorders include:
I. Disorders of vascular phase:
• Physiological: Devil's pinches in newborns
• Vasculitis: Meningococcemia, dengue, SLE, HSP
• Collagen defects: Scurvy, Ehlers-Danlos syndrome
• Miscellaneous: Hereditary hemorrhagic telangiectasia, Cushing disease, steroids
II. Disorders of platelet phase: (Ch 19.11)
• Quantitative defects (Thrombocytopenia)
- Idiopathic thrombocytopenic purpura
- Secondary thrombocytopenia
• Qualitative Platelet function defects
III. Disorders of coagulation (Ch 19.12)
• Inherited, e.g. hemophilia, von Willebrand disease
• Acquired, e.g. vitamin K deficiency, chronic liver disease
Diagnostic evaluation for bleeding disorder initially aims to differentiate between—(a) bleeding and clotting disorders (Table 19.19), and (b) inherited and acquired defects. Further investigations are needed to identify precise defect for rational therapy and genetic counseling. Detailed history must include: (a) age of presentation, (b) site of bleeding (superficial/deep), (c) onset of bleeding (spontaneous/post-traumatic), (d) past history of similar episodes, (e) family history of similar events (specially on maternal side), (f) history of drug intake, e.g. aspirin, NSAIDs, etc.. Menorrhagia may be the only manifestation of disorders like von Willebrand disease or platelet function defects in adolescent females.
Clinical examination should search not only the probable cause (e.g. chronic liver disease), but also for signs of concealed bleeding, e.g.
intracranial hemorrhage, which may be life-threatening.Hess test is a bed-side test to assess capillary fragility, seen in many bleeding disorders. In this, pressure is applied to the forearm with a BP cuff inflated between systolic and diastolic pressure for 10 minute. Appearance
ITP: Immune thrombocytopenic purpura
TCP: Thrombocytopenic purpura; VWD: von Willebrand disease; HDN: Hemorrhagic disease of newborn
of gt;15 petechiae within 5 cm diameter over forearm indicates increased capillary fragility. It is also positive in thrombocytopenia.
Laboratory investigations: While most cases may be identified on the four screening tests—BT, platelet count, PT and PTT (Table 19.20). Other useful investigations include:
• Complete blood counts with peripheral smear help to identify extent of anemia, involvement of other cell lines (leukemia, aplastic anemia) and platelet count/ function.
Absence of platelet clumps on smear indicates severe thrombocytopenia (lt;10,000-20,000#8725;mm3) while inadequate clumping despite normal platelet count indicates possible aggregation defects. Presence of large-size platelets indicates excessive peripheral destruction or Bernard-Soulier syndrome (Giant platelet syndrome).
• Platelet count differentiates between bleeding vs. clotting disorders and between thrombocytopenic purpura vs. platelet function defects.
• Ivy bleeding time (BT), is measured as time required for hemostasis after a superficial skin incision of 1-2 mm depth and ~5 mm length in forearm, with a BP cuff tied above the incision and pressure maintained at 40 mmHg. Normal value is 4-8 minutes. Prolonged BT indicates thrombocytopenia or platelet function defects.
• Platelet function tests usually include aggregation studies after addition of an agonist, e.g.
ADP, epinephrine, collagen, thrombin and ristocetin, to activate platelet-rich plasma. These tests aim to identify qualitative defects like Glanzmann's thrombasthenia. Clot retraction is defective in both thrombocytopenia and thrombasthenia.• Clotting profile: Various phases of clotting cascade are assessed as follows:
- Lee-White clotting time (CT) is too unreliable to have a diagnostic value, and may be normal (5-8 minutes) even in severe clotting defects.
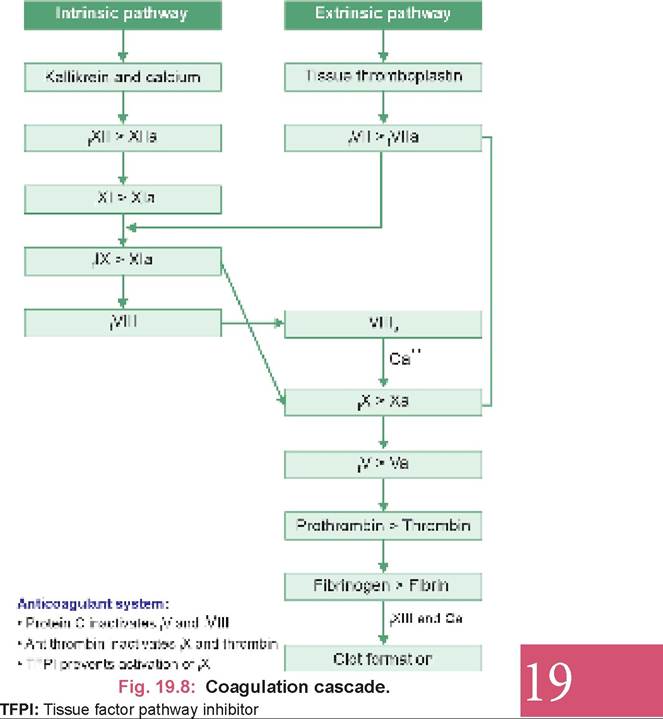
- Activated partial thromboplastin time (aPTT) measures intrinsic pathway of clotting cascade, with normal values ranging from 25-40 seconds (compare with control).
- PT (Prothrombin time) measures extrinsic pathway as well as common pathway, following the activation of tissue factor. Normal values are between 10-13 seconds (compare with control, denoted as quot;Prothrombin indexquot;).
- Thrombin time (TT) measures final step of the conversion of fibrinogen to fibrin, with normal value as 11-15 seconds. Prolonged TT indicates afibrinogenemia, hypofibrinogenemia or heparin therapy.
- Mixing studies differentiate between clotting factor deficiencies and presence of factor inhibitors. Correction of abnormal PTT by adding exogenous factor, i.e. normal plasma, indicates a clotting factor deficiency, while persistent abnormality suggests presence of fVIII, fIX or fXI inhibitors.
Mixing studies are also be used to differentiate between fVIII, fIX and fXII deficiencies. fVIII is present only in plasma but not in serum, while fIX is present in serum but not in plasma. fXI is present in both serum as well as plasma. Correction of abnormal PTT after addition of normal plasma (not by serum) or normal serum (not by plasma) indicates fVIII and fIX deficiency, respectively. fXI deficiency may be corrected by addition of both- normal plasma or serum.
- Specific clotting factor assays are used to establish the presence/severity of specific factor deficiencies.
- Urea solubility test is used to detect fXIII deficiency by abnormal solubility of blood-clot in 5M urea solution and short euglobulin lysis time.
19.11