MANAGEMENT OF SEVERE ACUTE MALNUTRITION
SAM is a major cause of mortality and morbidity and needs specialized care in a hospital or nutrition rehabilitation centers (NRC) - dedicated units in hospitals for nutritional therapy and support.
However, some cases of SAM do not need hospital care and may be managed at home under supervised care. Thus, the management of SAM may be broadly divided into: (a) facility-based care, and (b) community-based care, discussed in the following sections.A. Facility-based Care
Hospitalization is indicated in all cases of SAM (6-59 months) with following risk factors:
• Complicated SAM with life-threatening complications, i.e. infections, hypothermia, dehydration, electrolyte/ metabolic derangements, severe anemia, etc. (Table 6.6).
• Presence of severe edema
• Presence of danger signs of IMNCI (convulsions, altered sensorium, inability to drink/feed, persistent vomiting)
• Failure to pass appetite test
• Lack of reliable home care/supervision
In addition, all infants lt;6 months with SAM and/or those who are too weak or feeble to suckle, need hospitalization.
Appetite test aims to assess the extent of the loss of appetite. Children with good appetite, even with SAM, can be managed on outdoor basis in absence of other complications. It involves offering the child a measured amount of feed and assessing the unconsumed portion to calculate the intake.
• For children 7-12 months: Offer 30-35 ml/kg of catchup formula diet (Table 6.11). Child is considered to have good appetite, if she/he can consume gt;25 ml/kg.
• For children gt;12 months: Offer a specially prepared feed from local ingredients (mix roasted and grinded groundnut 1000 gm, grinded sugar 1120 gm, milk powder 1200 gm and coconut oil 600 gm and store in air-tight container in refrigerator; to be used within one week). To pass the appetite test (good appetite), child should
be able to consume gt;15 gm (wt lt;4 kg), gt;25 gm (wt 4-7 kg) and gt;33 gm (7-10 kg) of this feed.
Appetite test should be performed in a separate quiet area after explaining the purpose and procedure to the mother. The child should not have been fed in last two hours and must not be forced to take the feed. The test may take up to one hour and the remaining amount must be measured to assess the intake.
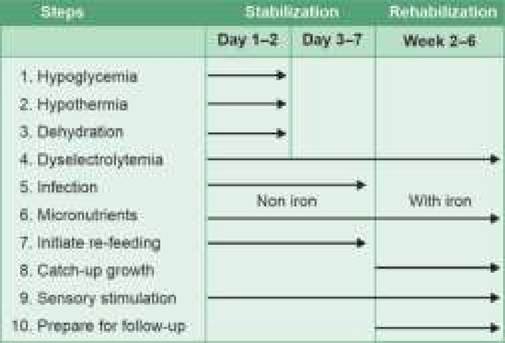
Fig. 6.6: Ten steps in management of SAM (WHO).
Ten steps of SAM management: Management of SAM may be broadly divided into three phases: (a) stabilization phase, (b) transition phase, and (c) rehabilitative phase.
• Stabilization phase (1-2 days) involves treatment of major medical complications and initiation of re-feeding with suitable starter feeds to promote normalization of metabolic function and nutrition- electrolytic balance.
• Transition phase (2-3 days) after stabilization, aims to ensure that the child is clinically stable before gradual switch-over from starter diet to catch-up diet.
• Rehabilitation phase (2-6 weeks) aims to promote rapid weight gain, stimulate emotional and physical development and prepare the child for discharge, after gradual switch-over on home diet.
WHO has proposed 10 essential steps in the management of SAM within a given timeframe (Fig. 6.6), as follows:
Step I. Treat and prevent hypoglycemia: All SAM children are at risk of hypoglycemia (blood glucose lt;54 mg/dl) and should be checked for blood glucose levels on admission. If it is not possible, hypoglycemia must be assumed to be present.
Asymptomatic hypoglycemia is more common and should be treated promptly by 50 ml of 10% dextrose/ sugar solution, fed orally or via nasogastric tube, followed by the first feed of starter F-75 formula (discussed later, Table 6.9) every two hours to prevent recurrence. First F-75 feed may be given as small volume (1/4th part of 2-hourly feeds) every 30 minutes, till the stabilization. blood glucose levels should be re-checked 2-hrly, till stabilized.
Symptomatic hypoglycemia with altered sensorium and/or seizures, should be treated promptly with IV dextrose 10% (5 ml/kg) as bolus, followed by oral dextrose/sugar solution or F-75 feed, as discussed earlier for asymptomatic hypoglycemia. Blood glucose levels should be rechecked 2-hourly, till stabilized.
Hypoglycemia can be prevented by frequent regular feeds, including at night along with periodic monitoring. Step II. Treat and prevent hypothermia: Hypothermia (rectal temperature lt;35.5°C) is more common in marasmus due to less subcutaneous fat. It may also indicate underlying hypoglycemia or infections. Blood glucose levels should be checked in all cases of hypothermia. Baby should be assumed as hypothermic, if rectal thermometer is not available and temperature is not recordable by skin thermometer.
Treatment of hypothermia involves: (a) gradual rewarming under radiant warmer/blanket or putting him/ her on the mother's bare chest for skin-to-skin contact, (b) frequent feeding, and (c) starting antibiotics as per step V. Rectal temperature should be monitored every 30 minutes, till it exceeds 36.5°C.
Prevention of hypothermia involves: (a) frequent 2-hourly feeding even during nights, (b) keeping the baby warm and well covered with mother and dry by changing wet-nappies as needed, and (c) avoiding prolonged cold-exposure for examination or procedures. Step III. Treat and prevent dehydration: Dehydration is common in malnourished children due to co-existent diarrhea/vomiting, poor oral intake and redistribution of body fluids. Severity of the dehydration is often overestimated in these cases and parenteral fluids should be avoided unless the patient is in shock. Conversely, dehydration may be missed in edematous children. Any SAM child with diarrhea must be presumed as dehydrated.
Mild to moderate dehydration is preferably treated with WHO-ORS, given orally or via nasogastric tube as 5 ml/kg every 30 minutes for first two hours, followed by 5-10 ml/kg/hr for maximum 12 hours, depending on the needs.
While IAP recommends use of WHO-ORS for this purpose, WHO recommends use of half-diluted ORS or Rehydration Solution for Malnutrition (ReSoMal) to rehydrate SAM children, except in cases of cholera or profuse watery diarrhea.ReSoMal, though rarely used, can be prepared by diluting one packet of WHO-ORS in 2 liters of water (instead of 1 liter) and adding 50 gm of sugar and 40 ml of specially prepared electrolyte-mineral solution. It should be used only under medical supervision in in-patient care.
All cases should be monitored for hydration by pulse rate, respiratory rate, urine output and stool/vomit frequency, every 30 minutes in first two hours and then hourly for next 6-12 hours. Oral fluids must be replaced with F-75 feeds in the same volume at 4, 6, 8 and 10 hours, if dehydration continues.
Parenteral fluid therapy is necessary in cases with shock, with a cautious approach due to risk of fluid overload. IV Ringer lactate or N/2 Saline in DW 5% is
preferred, given as 15 ml/kg in first hour and repeated after one hour (in responders), followed by switch-over to oral fluids. All cases should be closely monitored for signs of fluid overload, e.g. tachycardia, tachypnea, edema and puffy eyelids.
If the child fails to improve after the first hour of parenteral fluids, she/he should be assumed to have septic shock and treated with maintenance IV fluids (4 ml/kg/hr) along with fresh whole blood transfusion at 10 ml/kg slowly over 3 hours.
Dehydration can be prevented in a SAM child with watery diarrhea by feeding F-75 feeds (step 7) and replacing the stool losses with 50-100 ml of ReSoMal/ half-ORS after each watery stool. Breastfeeding should be encouraged in breastfed children.
Step IV. Correct electrolyte imbalance: Dyselectrolytemia is common in malnutrition due to poor intake, losses in diarrhea/vomiting and redistribution of body fluids, even in absence of clinical signs.
All malnourished children have excess body sodium due to renal retention, despite low or normal plasma sodium levels and should receive low-salt diet.
Hypertonic fluids should be strictly avoided.Hypokalemia is common due to redistribution of body fluids, which may be asymptomatic or presents with muscular weakness and abdominal distension. Asymptomatic hypokalemia can be treated with oral potassium supplements 3-4 mEq/kg/day for 2 weeks as commercial potassium chloride solution (20 mEq/ 15 ml),given mixed with feeds. In cases on IV fluids, potassium must be added to IV fluids as 2-3 mEq/kg/ day, after the child has passed urine.
Hypomagnesemia is common due to reduced muscle mass and may be corrected by oral magnesium supplementation as 0.8-1.2 mEq/kg. On day one, all malnourished children must receive single dose of IM magnesium sulfate (0.3 ml/kg, max 2 ml).
Hypocalcemia m ay be present due to low albuminbound fraction, but rarely needs to be treated as ionic calcium is usually normal.
Step V. Treat and prevent infections: Infections are common but may be difficult to recognize due to poor inflammatory response and absence of constitutional signs, e.g. fever. All cases of SAM on admission must be presumed to have infection and treated with empirical antibiotics. Presence of hypothermia, hypoglycemia, shock and bleeding tendencies indicates potentially serious underlying infection.
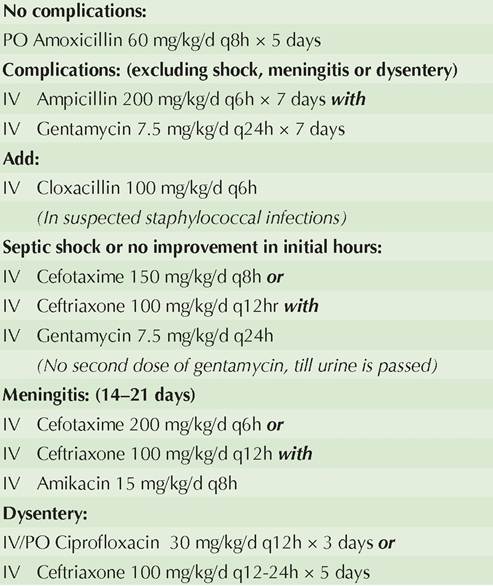
Choice of empirical antibiotics and duration of therapy varies with severity of sepsis and presence of complications (Table 6.8), which should be modified after culture reports. Some workers also suggest metronidazole (PO 30 mg/kg/d q8h 7 days) to cover anaerobic infections. Antimalarial therapy is indicated only if smear is positive.
TABLE 6.8: Antibiotic therapy in SAM
Step VI. Correct micronutrient deficiencies, which are common but often asymptomatic due to adaptive mechanisms.
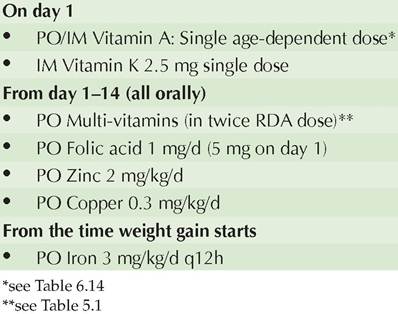
Vitamin A supplementation is indicated in age dependent single oral dose (2, 00,000 IU lt;1 yr, 1, 00,000 IV in 0.5-1 yr and 50,000 IU lt;6 mo) on admission.
However, in cases with clinical signs of deficiency, three doses on day 1, 2, 14 are required. Intramuscular administration is needed (half of the oral dose) in cases with severe anorexia, edematous malnutrition or septic shock. WHO recommends daily vitamin A supplements (5000 IU/day) and not the single dose therapy as above, except when feeds not fortified with vitamin A.Vitamin K (IM 2.5 mg) is also recommended as singledose on the day of admission.
Other vitamin-mineral supplements, except iron, must be given from the day of admission for at least 2 weeks (Table 6.9), either separately or as combined preparation. Multivitamin preparation should also contain vitamin A, C, D, E and B12 along with other minerals, in doses twice of the recommended dietary allowance.
Iron supplements should be delayed till the baby starts gaining weight and is on catch-up diet for at least 2 days, as it may be utilized by organisms for their metabolism and deteriorate the underlying infection. It should be continued for at least 2 months to replenish stores. Transfusion should be avoided due to potential risk of CCF, indicated only in cases with hemoglobin lt;4 gm or
TABLE 6.9: Micronutrient supplements in SAM
4-6 gm with respiratory distress. In them, whole blood may be transfused (10 ml/kg over 3 hour), along with IV furosemide (1 mg/kg) at the beginning of transfusion. Packed cells transfusion (5-7 ml/kg) should be used instead of whole blood in presence of CCF. All cases should be monitored or fluid overload. Blood transfusion should not repeated in next 4 days, if avoidable.
Step VII. Initiate re-feeding: Feeding should begin as soon as possible, though cautiously due to fragile physiological state and limited homeostatic capacity. Early feeding at this stage aims to provide sufficient energy and proteins for basic metabolic processes, without expectation of weight gain. However, these children have poor appetite and limited capacity to handle proteins, fats and solutes. Important considerations to initiate refeeding are as follows:
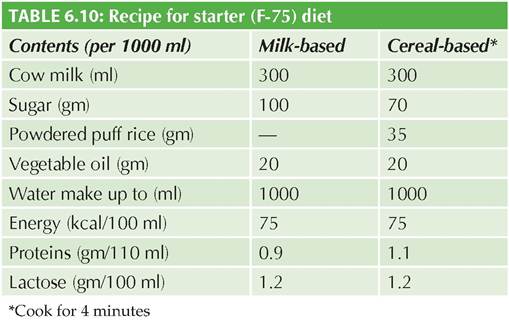
• Recommended dietary intake during this phase is~100 kcal/kg/d of energy, 1-1.5 gm/kg/d of proteins and 130 ml/ kg/d of fluids of actual weight (100 ml/kg/d fluid, if the child has severe oedema).
• Starter feeds must provide ~ 75 kcal and ~ 0.9 gm protein per 100 ml (F-75), which may milk-based or cereal-based, preparedly locally (Table 6.10).
• Frequency and volume of feeds depend on the acceptance. Usually, small and frequent (8-12/day) feeds are required in the beginning, given throughout the day, including in night. Volume of each feed may be increased gradually as the appetite improves.
• Oral feeds are preferable, though nasogastric feeding is indicated if the baby is unable to consume at least 80% of offered feeds.
• Breastfeeding should be encouraged ad libitum in breastfed cases, along with starter feeds.
• All cases should be monitored daily for body weight, losses in stools/vomiting and 24-hr intake, carefully assessing the feeds offered and leftovers.
Step VIII. Feeding for Catch-up growth: Once the appetite returns and child is stabilized, usually after a week, rehabilitation phase begins to rebuild wasted
tissues and ensure weight gain. Important considerations for catch-up diet during this phase are as follows:
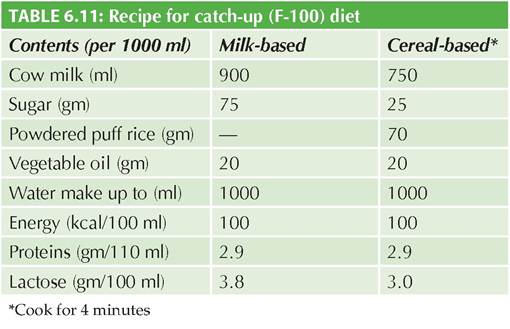
• Catch-up diet (F-100) must be relatively more energy- dense, containing ~100 kcal and 2.9 gm protein per 100 ml, which may milk-based or cereal-based, preparedly locally (Table 6.11).
• To being with, starter-formula feeds (F-75) must be replaced with the same amount of catch-up formula (F-100) for first two days, followed by gradually increasing the each feed by 10 ml, until some feed remains uneaten. Usual intake at this stage is expected to be ~30 ml/kg/feed or ~200 ml/kg/day.
• To begin with, child should receive at least 8 feeds/ day of catch-up formula. Gradually, some of these feeds may be replaced by ready-to-use therapeutic foods (RUTF, discussed later) or locally prepared therapeutic foods or modified family foods with comparable energy and protein concentration, e.g. khichri or halwa, to prepare the child for discharge on home diet. Breastfeeding should be continued ad libitum, in breastfed children.
• Child should be encouraged to eat as much as possible and offered more feeds next time, if finished everything. Frequency may be reduced gradually to 6 feeds/day, as the volume per feed improves. At the end of this phase, target is to give 200 calories ml/kg/day and 4-6 gm/kg/day of proteins, of actual weight.
• All cases should be monitored for daily weight gain, expected to be ~10 gm/kg/day. Child should be reassessed for underlying infection or psychosocial problems, if weight gain is inadequate. All cases should also be monitored for signs of heart failure.
• Infants lt;6 months should not given undiluted F-100 due to risk of solute overload and must be managed with breastfeeding and/or F-75.
Failure to respond during rehabilitation phase is defined as weight gain lt;5 gm/kg/day, while those with gain between 5 and 10 gm/kg/day are considered to have moderate response. Poor weight gain may be due to:
(a) inadequate feeding, (b) specific nutrient deficiencies, (c) underlying infection or systemic disease, and (d) emotional deprivation.
Failure to respond is further classified as primary failure when child fails to: (a) regain appetite by 4th day,
(b) start loosing edema by 4th days, (c) loose edema by 10th day, and (d) gain weight by at least 5 gm/kg by 10th day. Secondary failure denotes weight gain of lt;5 gm/kg/ day for three consecutive days in rehabilitation phase.
Step IX. Provide sensory stimulation and emotional support: Developmental delay and behavioral changes are common in SAM children. Emotional and physical stimulation is an integral part of management in these cases and includes: (a) tender and loving care, (b) cheerful and stimulating environment, (c) encouragement of physical activity, (d) maternal involvement in child care, and (e) structured play-sessions including language and motor activities with the help of toys, etc.
Step X. Prepare for follow-up after recovery: Most cases need ~10-15 days of hospitalization, while remaining part of rehabilitation phase may be completed at home, followed by periodic follow-up for 4-6 month to prevent recurrence. While preparing for the discharge:
• Child should be gradually switch-over from catch-up diet to regular family meals, in adequate quantity and appropriate quality.
• Mother must be trained to follow correct feeding practices, including need for breastfeeding, preparation of nutritious feeds and feeding frequently.
• Immunization must be completed for age.
• De-worming must be done with single oral dose of Albendazole 200 mg (400 mg for gt;2 yr).
• Follow-up plan must be shared with mother, who should also be trained to recognize signs which need immediate medical attention.
Criteria for discharge: WHO recommends that SAM cases should be discharged only after achieving: (a) Wt for Ht gt;-2 SDS/ z-score, (b) no edema for at least 2 weeks, and (c) MUAC gt; 12.5 cm. WHO does not recommend use of percentage weight gain as criteria for discharge. However, considering the patient-load, Government of India guidelines recommend that a SAM case can be discharged from the hospital if:
• has gained gt;15% of pre-admission weight with satisfactory gain for 3 consecutive days (gt;5 gm/kg/day),
• accepting adequately the nutritious foods that the mother can prepare at home,
• all infections and other medical complications have been treated,
• has been provided with micronutrients,
• has been fully immunized, and
• mother has been trained for good feeding practices and sensory stimulation at home. She must also be able recognize the signs which need immediate medical assistance.
On discharge, these cases should be transferred to the outpatient therapeutic program (OTP), discussed later, and must be followed up every 2 weeks in first month and then monthly thereafter until weight for height reaches gt;-1 Z/SD-score.
Re-feeding (Recovery) syndromes: While rarely seen at present due to the use of standard guideline-based management, children recovering from SAM are prone to develop many complications due to unmasking of subclinical nutrient deficiencies and should be carefully monitored for:
• Diarrhea due to relative lactase deficiency and other malabsorption states, precipitated by increased nutritional intake,
• Congestive cardiac failure due to shift of edema fluid in intravascular compartment, following high solute and protein diet,
• Un-masking of sub-clinical vitamin and mineral deficiencies, e.g. scurvy, zinc deficiency, due to disturbed adaptation.
Two well-defined clinical syndromes seen during the recovery phase are Kahn and Gomez recovery syndromes, probably caused by unmasking of subclinical nutrient deficiencies.
• Kahn's recovery syndrome is characterized by sudden onset of tremors and encephalopathy, probably due to unmasked deficiency of gamma aminobutyric acid (GABA)-a major neuroinhibitors.
• Gomez recovery syndrome is characterized by progressive abdominal distension, ascites, hepatomegaly and diarrhea, due to secondary malabsorption and dyselectrolytemia, e.g. hypokalemia.
B. Community-based Care
Generally, SAM is managed in hospitalization set-up while MAM is managed on outpatient basis. However, it is neither possible nor desirable to provide facility-based care to all SAM children in resource-limited settings. Community-based care or home-based care is a more feasible concept for the management of malnutrition in resource-limited settings and includes:
• Outpatient therapeutic program (OTP) for children with SAM but good appetite and no medical complications or those who have been prematurely discharged from the facility-based care.
OTP should aim to provide ~150 calories and 4 gm/ proteins per day till complete recovery, using frequent energy/protein dense meals either as read to use therapeutic food (RUTF) or home-based modified diet along with micronutrient supplementation. Children are followed-up weekly at an OTP site in a community setting, for periodic check-ups and replenishment of RUTF.
• Supplementary feeding program (SFP) for children with MAM or those who have been graduated from OTP. SFP provides for dry take-home rations and routine basic treatment.
However, facility-based care is a must for children with SAM and poor appetite (failed appetite test) or associated medical complications.
Ready-to-use therapeutic food (RUTF) is an energy- dense mineral/vitamin-enriched food, specifically designed to treat SAM cases under OTP care. Although similar to F-100 in formulation, RUTFs have been shown to promote faster rate of recovery.
An ideal RUTF should be: (a) caloric dense with adequate proteins, vitamins and minerals, (b) palatable and acceptable, (c) affordable cost, (d) stable with long- shelf life, and (e) easy to administer, and (f) available in suitable packs to avoid wastage.
RUTF is an oil-based preparation that contains a little water to make it microbiologically safe for storage. Since it is eaten uncooked, RUTF is also time-saving with no loss of micronutrients during cooking.
While commercial RUTFs are available in some countries, low-cost RUTF can be prepared locally using simple and easily available ingredients, e.g. whole milk powder (30 gm), peanut butter (25 gm), sugar (28 gm) and vegetable oil (15 gm), fortified with micronutrients. Each 100 gm of this RUTF provides 520-550 calories, including 45-60% from fats and 10-12% from proteins. It can be stored for 3-4 months without refrigeration and should be fed directly with plenty of water.
However, RUTF should not be confused with ready to-use foods (RTUF), e.g. maggi noodles, and should be used only for therapeutic purpose and not as supplementary food, for limited time period (4-8 weeks) until the child recovers from SAM.
RUTF vs Modified home diet: Government of India does not approve use of RUTF and favours the use of modified home diet or locally prepared therapeutic diets for these children, along with supplementary nutrition. Several locally prepared therapeutic diets have been developed and being used for community-based management of acute malnutrition programs of different states, e.g. Telangana. Some states provide for take-home ration program at community centers to provide 150-180 cal/ kg and 3.5-5.5 gm/kg of proteins.
Amylase rich foods (ARF) are easily digestible and enriched sources of proteins and vitamins, prepared by soaking common cereals or pulses in water for 12 hours
gt; sprouting by wrapping in a moist cloth for 48 hours,
gt; drying gt; roasting gt; grueling to make porridge grinding, before storage. One teaspoonful (5 gm) of this powder may be added in each infant food after cooking. On soaking, the amylase breaks down grain-starch into easily-digestible maltodextrins, reducing the viscosity and bulk of diet. Germination also enhances vitamin content.
6.1.6