Management of Spinal Deformity
Severe spinal deformity and progressive NMD lead to multiple problems, including poor sitting balance, difficulty with upright seating and positioning, pain, difficulty in parental or attendant care, and potential exacerbation of underlying restrictive respiratory compromise (Fig.
12.18). Severe scoliosis and pelvic obliquity can, in some instances, completely preclude upright sitting in a wheelchair. The management of spinal deformity and progressive neuromuscular disease has recently been reviewed (17). Populations at risk for scoliosis include DMD, autosomal-recessive LGMD, congenital muscular dystrophy, FSHD muscular dystrophy, congenital myotonic muscular dystrophy, spinal muscular atrophy II and III, and Friedreich's ataxia. While previous estimates of incidence of severe scoliosis in DMD approached 80% to 90%, recent evidence suggests that corticosterorids (specifically deflazacort) may significantly decrease the incidence of severe progressive scoliosis in DMD (22).Close clinical monitoring is essential for children with NMD at risk for scoliosis. Curves may progress rapidly during the adolescent growth spurt, and children need to be monitored every three to four months during this time, with clinical assessment and spine radiographs if indicated. In addition, patients who are likely to require surgical arthrodesis at some point should be monitored with pulmonary function tests every six months. A forced vital capacity falling below
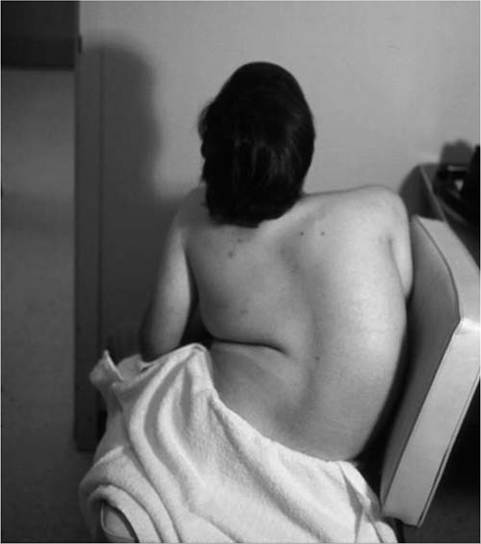
Figure 12.18 Scoliosis in Duchenne muscular dystrophy compromising long-term comfortable supported sitting in a power wheelchair.
30% to 40% of predicted does not contraindicate surgery (28), but is associated with increased perioperative morbidity and likely the need for prolonged noninvasive ventilatory support during the postoperative recovery period (27).
Thus, there is often a critical window of time where the spinal deformity is evident and likely to continue to progress and the restrictive lung disease is not of a severity that would contraindicate surgery or be associated with perioperative complications.The management of spinal deformity with orthotics is ineffective in DMD and does not change the natural history of the curve. Spinal orthoses are often reported to be uncomfortable and poorly tolerated by DMD patients. Furthermore, vital capacity potentially can be lowered with constrictive orthoses. On the other hand, in neuromuscular diseases with spinal deformity beginning in the first decade of life, such as SMA, congenital muscular dystrophy, congenital myotonic muscular dystrophy, some congenital myopathies, and congenital myasthenic syndromes, spinal bracing is generally used to improve sitting balance in patients who are unable to walk. In addition, spinal orthotics are employed in these younger patients in an attempt to halt curve progression until children are 10 to 11 years of age, when a single posterior spinal arthrodesis procedure is sufficient. Children younger than the age of 10 generally require both anterior and posterior spinal arthrodesis because of continued spinal growth, which decreases in rate after age 11 to 12. If a younger child has a severe progressive curve and severely compromised pulmonary function, a posterior fusion may be considered, with acceptance of the fact that some rotational “crank shaft deformity” will ensue.
Spinal arthrodesis is the only effective treatment for scoliosis in DMD, autosomal-recessive LGMD, congenital muscular dystrophy, congenital myotonic muscular dystrophy SMA, and Friedreich’s ataxia. The decision to pursue posterior spinal instrumentation involves a consideration of the severity of the restrictive lung disease, severity of the cardiomyopathy, severity and flexibility of the spinal deformity, and likelihood that the spinal deformity will continue to progress. Surgical spinal arthrodesis should be deferred to a later date in marginally ambulatory patients with LGMD, congenital muscular dystrophy, FSHD, and spinal muscular atrophy type III, as these individuals may use significant lumbar lordosis during gait to compensate for hip extensor weakness.