MECHANICAL BIRTH INJURIES
Incidence of mechanical birth injuries in India is estimated to be ~ 2-7/1000 live births, accounting for ~ 2-3% of neonatal deaths (Table 12.19). Some important mechanical birth injuries are as follows:
Caput succedaneum is a diffuse, edematous and often ecchymotic swelling of the soft tissue covering the presenting part, e.g.
scalp or face, which may extend across midline and sutures. It disappears spontaneously within a few days of life and no treatment is necessary. Cephalohematoma is a sub-periosteal hemorrhage, essentially limited by sutural lines and presenting as unilateral (or rarely bilateral) soft and fluctuant scalp swelling. Swelling usually appears after a few hours of birth due to slower bleed in confined space, enlarges for few days and reabsorbs spontaneously in 3-6 weeks.Incidence: It is seen in 1-2% of deliveries, more common in obstructed labor, forcep deliveries or vacuum extractions.
Diagnosis is obvious clinically, but may be confirmed on X-ray skull that reveals subperiosteal bleed and rarely, an underlying linear skull fracture (Fig. 12.7).
D/D includes caput succedaneum (Table 12.20) and cranial meningocele (pulsatile, increases on crying, underlying bony defect on X-ray).
Complications are uncommon but include—(a) anemia, (b) hyperbilirubinemia, (c) infection, if erroneously aspirated.
Management: Aspiration or surgical drainage is contraindicated, to avoid the risk of infection. No intervention is needed in small hematomas, though babies with large swellings should be observed and treated for complications, e.g. severe anemia or hyperbilirubinemia.
Brachial plexus injuries are common in large babies, specially when excessive lateral traction is applied to deliver shoulder in vertex deliveries or extended arm in breech deliveries.
Clinically, these injuries may present as upper-plexus (Erb-Duchenne paralysis) or lower-plexus (Klumpke's paralysis) injury or both.
• Erb-Duchenne paralysis, i.e. injury to upper roots of brachial plexus (C5_6) is characterized by:
- Abnormal limb position with adducted and internally rotated arm with pronated forearm (Policeman stick appearance), due to weakness of abductors, external rotators and supinators (Fig. 12.8A).
- Asymmetrical Moro's reflex (d/d fracture, osteo- myelitis/ arthritis, dislocation)
TABLE 12.19: Common mechanical birth injuries
[*] Cranial injuries
Caput succedaneum
Cephalohematoma
Skull fractures (linear/depressed)
Intracranial hemorrhage
• Cervical injuries
Cervical spinal injuries
Sternocleidomastoid tumor
• Peripheral nerve injuries
Brachial plexus injury
Erb-Duchenne paralysis
Klumpke's paralysis
Phrenic nerve injury
Facial palsy
• Limb injuries
Fractures (clavicle, humerus, femur)
Dislocation of upper femoral epiphysis
• Visceral injuries
Liver (subcapsular hematoma)
Splenic rupture/hematoma
Adrenal hemorrhage
• Superficial Soft-tissue injuries
Skin abrasions, laceration, ecchymosis Genitals: Scrotal hematoma, hematocele Eye: Subconjunctival hemorrhage Retinal/vitreous hemorrhage
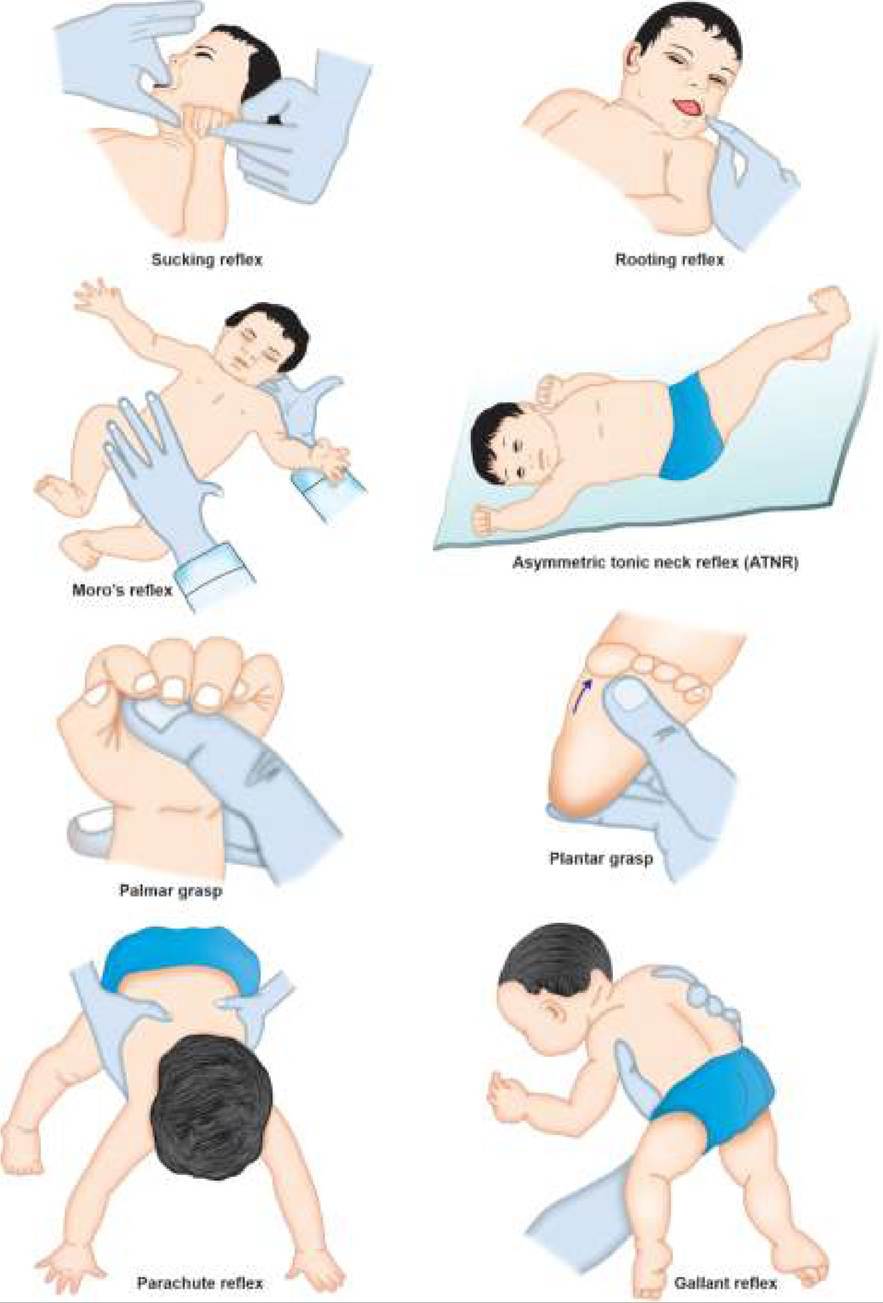
Fig. 12.7: Cephalhematoma: (A) Clinical appearance; (B) X-ray skull.

Figs. 12.8A and B: Brachial plexus injury: (A) Erb's palsy; (B) Klumpke's palsy.
- Normal power in forearm (except pronation) and hands with preserved grasp reflex
- Associated ipsilateral diaphragmatic paralysis due to phrenic nerve palsy (C3_5) in some cases.
• Klumpke's paralysis, due to lower-plexus injury (C7~g
T1) is relatively rare, presenting with:
- Weakness of wrist and hand movements with abnormal position (Accoucher's grip) (Fig.
12.8B)- Absent grasp reflex.
- Associated Horner syndrome (ptosis and miosis on affected side) due to injured T1 sympathetic fibres.
Management of brachial plexus injuries involves-(a) intermittent immobilization with splints in neutral position to prevent contractures during first 1-2 weeks, and (b) gentle massage with increasing range of motion exercises after 7-10 days. Recovery is unlikely beyond 6 months, when neuroplasty or nerve grafting must be considered.
Prognosis depends on whether the nerve fibers are merely injured (recovery in 2-3 months) or truly lacerated (permanent functional loss). Upper plexus injury has better prognosis than lower plexus injury. A intact gasp reflex suggests gt; 80% chances of recovery.
Skull fractures are common during breech or instrumental deliveries and may be linear or depressed. Some fractures may be associated with intracranial bleeding. No treatment is necessary for linear fractures without intracranial hemorrhage, while depressed fractures need neurosurgical assessment.
Clavicular fractures are most common bony injuries in macrosomic babies, delivered with shoulder or breech presentation. These babies present with restricted movement of affected arm (pseudoparalysis) with asymmetric Moro's reflex. No intervention is required except splinting and healing usually occurs in 2-4 weeks. Intracranial hemorrhage in newborns may be broadly divided into 2 types:
a. Subdural, epidural or subarachnoid hemorrhage, are more common in term newborns, usually caused by (a) mechanical head injury in obstructed labor, precipitate deliveries or forceps application, (b) bleeding disorders, e.g. DIC, immune thrombocytopenia, etc. and (c) intracranial vascular malformations.
These cases usually present with recurrent seizures, progressive head enlargement with bulging fontanels and anemia in late neonatal period. Diagnosis may be confirmed on USG or CT scan. Surgical evacuation of hematoma is indicated only in symptomatic cases.
b. Intraventricular/periventricular hemorrhage, is mostly seen in preterms with birth asphyxia, discussed earlier in Ch 12.10.1.
Sternocleidomastoid tumor (Torticollis) is actually a sub-facial or intramuscular hematoma in sternocleidomastoid muscle due to over-stretching and laceration of muscle fibers during delivery of impacted head in breech/ shoulder deliveries. Some cases are also thought to be hereditary or in utero muscle infection.
Clinically, these cases present on 10th-14th day with:
• A well-circumscribed, non-tender small mass (1-2 cm) over mid-sternocleidomastoid muscle, which gradually enlarges for 2-4 weeks, before regressing completely by 6-g months (Fig. 12.9).
• Torticollis with head tilted on same side and chin elevated and rotated on opposite side. Torticollis usually disappears with mass, but may persist for many years due to residual scarring and leads to secondary deformities, e.g. craniofacial asymmetry, scoliosis and gaze abnormalities.
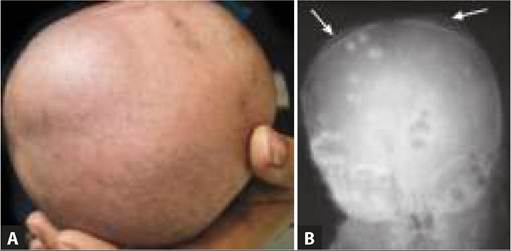
Fig. 12.9: Sternocleidomastoid tumor.
Treatment includes frequent gentle over-stretching of the neck on opposite side (taught to mother) in early months and bed-time splinting in corrected position. Surgical lengthening by division of sternal portion of muscle is indicated only in persistent torticollis beyond 6-8 months.
12.11