Motor Neuron Disorders
Spinal muscular atrophy (SMA) is perhaps the most common lower motor neuron disorder causing infantile hypotonia. The predictive value of needle EMG in the diagnosis of SMA has been established (36-39), but the need for electrodiagnostic studies has diminished over the years, given the 95% or greater sensitivity of SMN gene studies.
As SMA remains an important consideration in infantile hypotonia, a review of the ele- crodiagnostic findings is useful.The findings in this motor neuron disorder have largely been consistent with motor axonal loss, denervation, and (among persons less severely affected) reinnervation. Traditional electrodiagnostic criteria for motor neuron disease are not suitable for patients with childhood SMA. For example, Buchthal (41) found that many infants with SMA did not meet strict criteria for motor neuron disease. If clinical findings suggest SMA, study of at least two muscles innervated by different nerve roots and peripheral nerves in at least three extremities is indicated (42). In the infant, spontaneous activity may be more readily determined with study of muscles that are not as commonly recruited, such as the vastus lateralis, gastrocnemius, triceps, and first dorsal interosseous. Recruitment and motor unit characteristics can be assessed in muscles that are readily activated, such as the anterior tibialis, iliopsoas, biceps, and flexor digitorum sublimis (42). The paraspinals are usually not studied due to poor relaxation, and the experienced pediatric electrodiagnostic medicine consultant usually defers needle evaluation of the tongue in the hypotonic infant.
Although some authors (43) have described high- density fibrillation potentials in infants with poorer outlook, most studies have not demonstrated abundant fibrillation potentials in the infantile form (42,44,45). In SMA III, the incidence of fibrillation potentials ranged from 20% to 40% in one series (46) to 64% in another (47).
The incidence of fibrillation potentials in SMA type III does not approach the level seen in SMA type I. In addition, spontaneous activity has been more frequently observed in the lower extremities than upper limbs and proximal more than distal muscles in SMA type III (46). The degree of spontaneous activity has not been found to be independently associated with a worse prognosis in SMA (39). Fasciculations are uncommonly observed in SMA type I and appear more commonly in SMA types II and III (42,43,45). In younger patients, fasciculations are difficult to distinguish from spontaneously firing MUAPs. In relaxed muscles, some motor units exhibit a spontaneous rhythmic firing (43, 44, 45).Voluntary MUAPs frequently fire with an increased frequency, although recruitment frequency may be difficult to determine consistently in infants. Compared to age-matched norms, MUAPs show longer duration, particularly in older subjects, and higher amplitude; however, a bimodal distribution may be seen with some concomitant low-amplitude short duration potentials (44). Large-amplitude, long-duration MUAPs may be absent in many infants with SMA type I but more commonly observed in SMA types II and III (42). The percentage of large-amplitude MUAPs increases with the duration of the disease (46). Other signs of reinnervation, such as polyphasic MUAPs, may be observed in more chronic and mild SMA. These polyphasic MUAPs may include late components such as satellites or linked potentials. There may also be temporal instability of the waveform observed in individual MUAPs. Reduced recruitment (an incomplete interference pattern) with maximal effort is perhaps the most consistent finding in all SMA types (Fig. 7.7). In one series (39), the amplitude of MUAPs and degree of decrement in recruitment pattern were not individually associated with worse prognosis.
Motor nerve conduction velocities and CMAP amplitude have been shown to be reduced in many patients with infantile SMA.
The degree of motor conduction slowing (if present) tends to be mild and greater than 70% of the lower limit of normal (45,47-50). Reduction of motor conductions to less than 70% of the lower limit of normal is described as an exclusionary criterion for SMA (51). The mild slowing of motor conductions is present to the same degree over distal and proximal segments as determined by M- and F-waves responses (49). The slowing of conduction is generally seen in those with correspondingly low-amplitude CMAPs and is thought to be due to selective loss of the fastest conducting fibers from large motor units. Alternatively, arrested myelination in utero has been proposed to explain this slowing in motor conduction noted in some SMA cases at birth (39). Survival has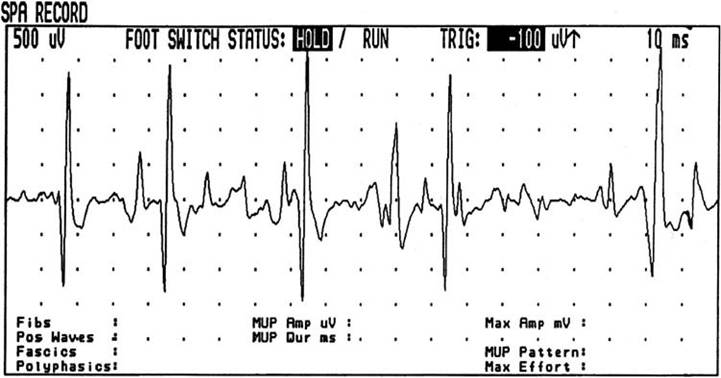
Figure 7.7 Incomplete or reduced interference pattern in spinal muscular atrophy type II. Note the large amplitude motor unit action potential (3,000 μV) firing at 25 Hz.
been found to be longer for those SMA infants with normal motor conduction velocities over a distal segment (39). Significant reductions in CMAP amplitudes have been frequently reported in SMA types I-III (39,42,47). Kuntz (47) reported a tendency toward greater reductions in CMAP amplitude among patients with earlier age of onset and shorter survival.
Sensory nerve conduction studies (NCSs) in SMA show essentially normal sensory conduction velocities and sensory nerve action potential (SNAP) amplitudes. Significant abnormalities in sensory studies exclude a diagnosis of SMA (51), while minor abnormalities in sensory conduction velocities have infrequently been noted in SMA (48,52,53). Such rare sensory abnormalities have not been reported in SMA patients with diagnostic confirmation by molecular genetic studies.