neurocysticercosis
Neurocysticercosis (NCC) is the commonest parasitic infection of CNS, caused by the invasive intermediate stage of T. solium (pork tapeworm), with formation of asymptomatic or symptomatic cysts in the brain or spinal cord (Ch 10.37.4).
Etiopathogenesis: NCC is caused by ingestion of parasitic eggs, present in soil, water or over the contaminated body of intermediate hosts, e.g. dogs, pigs or cattles (feco-oral route). Some of these eggs convert to an invasive form and cross the gut wall to spread hematogenously in different tissues, mainly brain and muscles.
Lodgement of these eggs in tissues produces tiny (2-5 mm) cysts containing single juvenile parasite, i.e. protoscolex. These cysts pass through four stages, i.e. vesicular, colloidal vesicular, granular nodular and calcified stage and do not provoke immune response as long as they are viable. However, degeneration of these cysts either in natural course after 5-10 years or after therapy, provokes strong host response and cysts clear up by complete resorption or calcification.
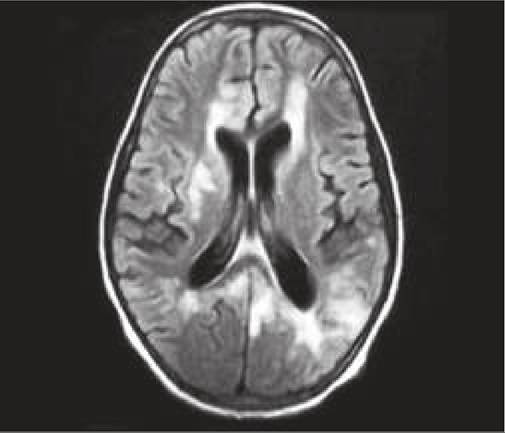
Fig. 18.16: Neurocysticercosis - Starry sky appearance on CT. Inset: protoscolex on MRI.
Clinical manifestations depend on the location of cysts as well as host response. Most of these cases remain asymptomatic. Symptomatic cases usually present either as ICSOL with recurrent seizures or hydrocephalus, or as cysticercal encephalitis with raised ICP.
Rare manifestations include focal motor deficits, signs of meningeal irritation due to meningeal cysts and compressive myelopathy due to spinal cysts. Rarely, cysts may also be present in other tissues, e.g. eyes (impaired vision), skin (palpable under the skin) or in skeletal/ heart muscles (myositis/carditis).
Diagnosis: Usually rests on:
• CT scan showing single or multiple cysts as ringenhancing lesions with protoscolex (hyperdense dot within cystic lesion or hole-with-dot appearance), with or without contrast enhancement or calcification.
Multiple cysts typically provide Starry-sky appearance (Fig. 18.16). Intraventricular cysts may be missed on CT. Calcified lesions appear as hyperattenuating nodule without perilesional edema/ enhancement.• MRI with contrast enhancement is a better imaging tool showing hyperintense lesion in T1 and hypointense in T2 images with pathognomonic protoscolex. Cysts are Usually lt;2 cm in size lesion with well-defined thin rounded walls located near the grey-white matter junction or basal ganglia. Uncommon locations include the posterior fossa, subarachnoid spaces, intraventricular space, and spinal cord.
Though not required for diagnosis, serological ELISA- blot test is sensitive in 90% cases, being false-negative in solitary small or calcified lesions. Stool examination for eggs is positive in lt;25% cases.
D/D: NCC needs to be differentiated from other causes of ICSOL. Closest d/d includes tuberculoma, based on MRI findings as follows:
• Smaller size of lt;1-2 cm in NCC vs large, confluent lesions in tuberculoma.
• Well-defined thin and rounded cyst walls in NCC vs thick, irregular walls in tuberculoma.
• Presence of scoleces within the cysts vs hypointense core (T2 images) in tuberculoma.
• Absence of marked perilesional edema, mass-effect or basal meningitis in NCC.
• MR spectroscopy showing multiple amino acid peaks with elevated acetate/succinate ratio in NCC vs lipid peak with elevated choline/creatinine and choline/ NAA ratio in tuberculoma.
Treatment of NCC includes anti-cysticercal therapy, steroids and anticonvulsants as follows:
• Specific anti-cysticercal therapy: PO Albendazole (15 mg/kg/day q12hr) for 10-14 days is the drug of choice for one or two viable cysts from day 3 onwards of steroid therapy (discussed below) while PO Albendazole along with Praziquantel (PO 50 mg/ kg/d) for 10-14 days is recommended for more than two viable cysts.
Anti-cysticercal therapy is not recommended in acute stage with multiple lesions (gt;5) or cysticercal encephalitis to avoid worsening of cerebral edema and raised ICP.
• Steroids (PO prednisolone 2 mg/kg/day q8hr) should be started 2-3 days before specific therapy, as sudden worsening of symptoms due to host response against dying parasites due to antihelminthic drugs is likely in initial phase. Steroids should continue for minimum 2 weeks. IV Dexamethasone (0.6 mg/kg/d) or methylprednisolone (30 mg/kg/d) is preferred in cysticercal encephalitis for 3-5 days, followed by gradual tapering.
• Anticonvulsant therapy is not required in absence of seizures, while six months of ACT is recommended for single lesions, if lesion resolves on follow-up. Those with persistent lesions or calcifications require minimum 24 months of ACT.
• Repeat neuroimaging is recommended after 6 months. For persistent lesions there are two options - either to repeat the same dose of albendazole or the concurrent administration of albendazole with praziquantel.
• Surgical interventions for hydrocephalus or removal of cysts blocking CSF pathway is rarely necessary.
18.13
More on the topic neurocysticercosis:
- INTRACRANIAL INFECTIONS
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025