NON-HODGKIN'S LYMPHOMA
NHL is a heterogeneous group of lymphoid malignancies, which primarily originate from lymphocyte precursors of T, B or indeterminate cells.
Unlike HD, NHL is more common in young children, usually presents as extra-nodal or generalized disease from the outset and carries relatively poorer prognosis, if not treated timely and adequately.
Epidemiology: Incidence of NHL increases with age, with maximum cases between 7 and 10 years. It is more common in males (3:1).
Etiology: While exact etiology is unknown, important associations have been found between NHL and—(a) EBV infection in Burkitt's lymphoma, (b) immunodeficiency states, e.g. AIDS, (c) chronic persistent antigenic stimulation in infections, and (d) chromosomal translocations involving proto-oncogenes or T-cell receptor genes, which regulate their production.
Some pathological subtypes have specific cytogenetic aberrations, e.g. (t8:14) translocation in 90% cases of Burkitt lymphoma.
Pathology: Childhood NHL are divided into 4 major histological types:
a. Lymphoblastic lymphoma or LL (30%), from immature T or B lymphocytes,
b. Burkitt lymphoma or BL (40%), usually of mature B cell origin,
c. Diffuse large B cell lymphoma or DLBCL (20%), with various subtypes, also usually of mature B cell origin,
d. Anaplastic large cell lymphoma or ALCL (10%), from mature T or B cells.
Lymphoblastic lymphoma is often indistinguishable from ALL, though presence of gt;25% blast cells in bone marrow is arbitrarily considered as suggestive of leukemia.
Clinically, Childhood NHL usually presents as extra- nodal disease with rapid growth and distant metastasis to bone marrow and CNS. About two-third of cases have widespread disease at the time of diagnosis. Clinical manifestations depend on the site of tumor and extent of involvement, which in turn depends on histological type.
• Abdominal mass is the commonest presentation in
NHL, specially in Burkitt lymphoma, with pain, intestinal obstruction, ascites, hepatosplenomegaly and obstructive jaundice.
• Mediastinal mass is the second commonest presentation (Fig. 20.2), especially in LL, with airway obstruction, pleural effusion, SVC syndrome and cervical lymphadenopathy.
• Spinal mass may present with severe backache, neurological deficit and raised intracranial pressure.
• Some cases may present with CNS, bone marrow, testis and skin involvement at the time of initial diagnosis.
Diagnosis depends on—(a) lymph node histology with immunophenotyping, (b) assessment for spread of disease by bone-marrow biopsy, CSF examination and
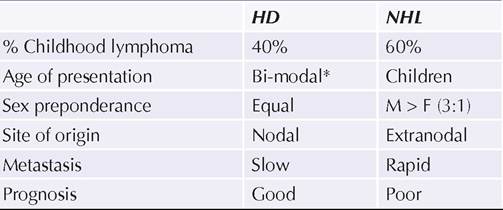
Fig. 20.2: Mediastinal mass in NHL.
imaging studies, e.g. USG abdomen, CT chest, PET scan, etc. Less than 20% blasts cells on bone marrow virtually rules out leukemia.
Other important investigations include renal and liver function tests, S. uric acid (to detect tumor lysis syndrome, common in NHL) and S. LDH levels.
St. Jude staging system (Murphy's classification) is commonly used to stage NHL for treatment and prognosis purpose (Table 20.10).
Treatment: Chemotherapy is the mainstay of treatment for childhood NHL, as it is considered a disseminated disease from the time of diagnosis. However, options differ as per histological type.
• BL or DLBCL are usually treated with 6 cycles of COMP regimen (Cyclophosphamide, Oncovin, i.e. vincristine, Methotrexate and Prednisolone), over 4-6 months, with gt;90% cure rate. Addition of Rituximab- an Anti-CD20 monoclonal antibody, is known to improve outcome in adults, and perhaps also in children with NHL. Other regimens, e.g. MCP842, LMB96 are also used in these cases.
• Localized or advanced LBL required longer-duration chemotherapy for 12-24 months (BFM-90 protocol), similar to that for ALL, including CNS prophylaxis with intrathecal methotrexate or cranial irradiation.
Survival rate is 60-80%. Relapses are common and need to be treated more intensively.• Advanced ALCL with localized disease may be managed with surgical resection alone, though most cases require chemotherapy with various protocols. Optimum therapy in these cases is controversial with lower cure rate, i.e. 50-70%. CNS prophylaxis with intrathecal methotrexate is also indicated, but cranial irradiation is generally avoided.
Tumor lysis syndrome is very common during initial phase of chemotherapy in NHL due to larger cell mass, which needs to be prevented by appropriate hydration and alkalinization of urine.
TABLE 20.10: St. Jude staging system for NHL
Stage I:
• Single extra-nodal or nodal tumor, except of mediastinum or abdomen
Stage II:
• Multiple nodal/extra-nodal tumor, with/out lymphnode involvement, on same side of diaphragm or
• A resectable primary GIT tumor, with/without involvement of mesentric nodes only
Stage III:
• Extra-nodal/nodal tumors on both sides of diaphragm, or
• Primary intra-thoracic tumors, or
• Extensive primary intra-abdominal disease, or
• Para-spinal or epidural tumors
Stage IV:
• Any of the above with CNS/marrow involvement
Surgery has limited role in NHL, except for diagnostic biopsy and intestinal complications, e.g. obstruction, perforation or bleeding.
Radiotherapy is avoided in most cases due to adverse effects, except in mass-effect emergencies, e.g. SVC compression or ureteric obstruction.
Prognosis depends on stage and histological type of disease. Bad prognostic indicators include—(i) advanced clinical disease, (ii) CNS or bone marrow involvement at the time of diagnosis, and (iii) large tumor mass. Relapses are more common in non-LBL types, which need to be treated with more intensive chemotherapy or bone marrow transplant.
20.3
More on the topic NON-HODGKIN'S LYMPHOMA:
- LYMPHOMA
- Hodgkin Lymphoma
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Immunodeficiency
- Macrovascular Complications of Diabetes Mellitus