Outcome Measures
Children with cerebral palsy often change over time, due either to growth and development or as a result of treatment. Various means of determining change may be employed. Subjective evaluations that ask the child, parent, or therapist their opinion are most commonly used.
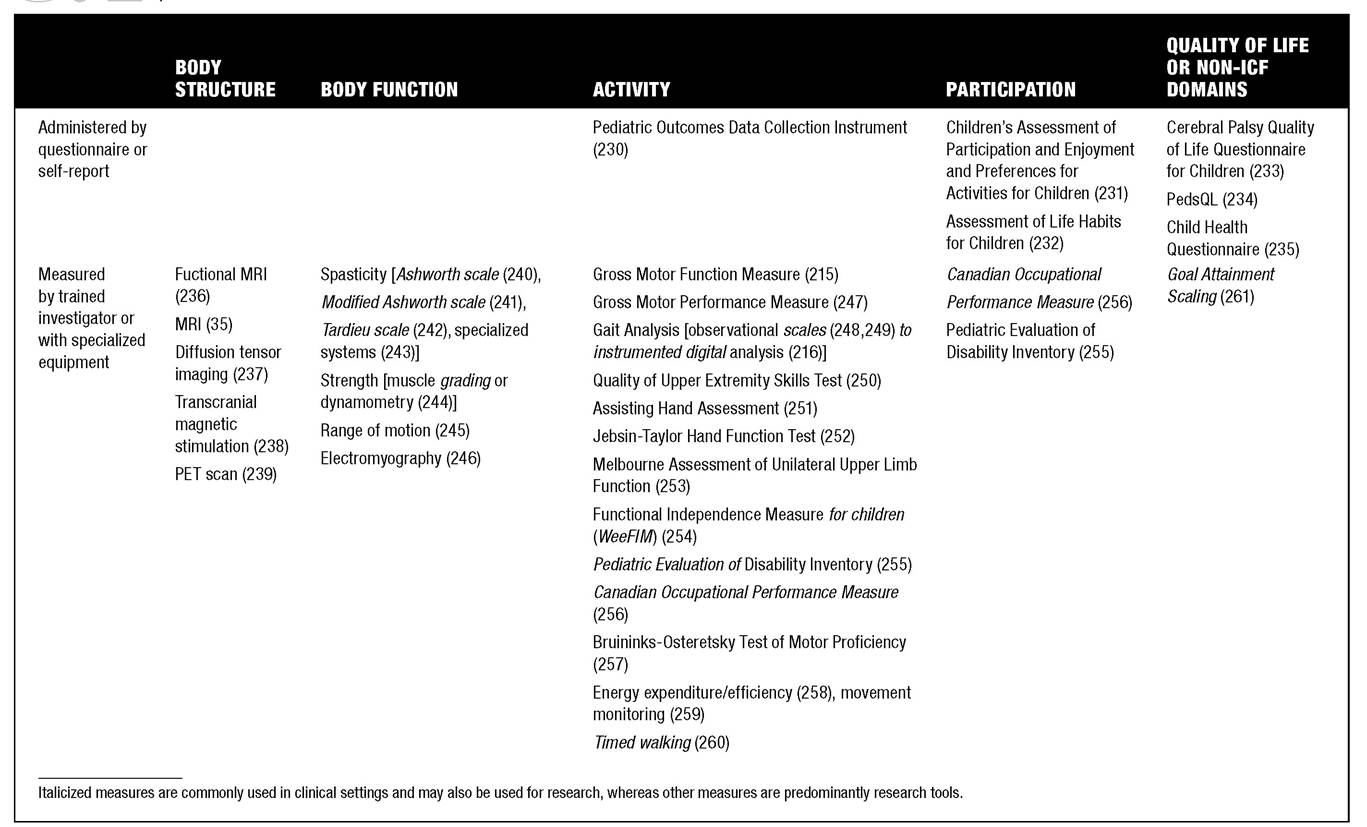
Occasionally, more quantified techniques are employed, particularly in research settings, although clinical use also occurs.Outcome measures may best be classified by the domains they seek to measure and the methods of assessment. Using the International Classification of Functioning, Disability, and Health—Children and Youth Version (ICF-CY) (214), measures can be divided into those that define body functions and structures, activity, or participation (Table 8.4).
Body Structure and Function
When considering children with cerebral palsy, few outcome measures directly relate to body structure. Imaging such as functional MRI or physiologic measures like transcranial magnetic stimulation or electromyography could be considered in this domain. Because very few interventions for cerebral palsy are expected to alter body structures, such as brain tissue, these types of outcome measures are seldom employed. Many outcome measures for cerebral palsy address body function. Body function is assessed with spasticity measurement (Ashworth, modified Ashworth, and Tardieu scales, or specialized measurement systems), strength measurement (muscle grading or dynamometry), or range of motion.
Activity
Because many interventions for cerebral palsy are intended to reduce activity limitation, a wide range of outcome measures are specific for this ICF domain. Common assessments of gross motor function and walking include the Gross Motor Function Measure and Gross Motor Performance Measure as well as gait analysis, ranging from observational scales (Physicians Rating Scale) to instrumented digital kinematic analysis.
Fine motor may be assessed with the Quality of Upper Extremity Skills Test, Assisting Hand Assessment, Jebsen-Taylor Hand Function Test, and Melbourne Assessment of Unilateral Upper Limb Function, among others. More global functional measures include the Functional Independence Measure for Children (WeeFIM), the Pediatric Evaluation of Disability Inventory, the Pediatric Outcomes Data Collection Instrument, and the Bruininks-Oseretsky Test of Motor Proficiency. Assessment of energy expenditure or efficiency, timed walking tests, and movement monitors are also used to assess the domain of activity in children with cerebral palsy.Developmental assessments are generally wide in scope and used more frequently in younger children. These include the Peabody Developmental Motor Scales, Battelle Developmental Inventory, Denver II, Bayley Scales of Infant Development, and Revised Gesell Developmental Schedule.
8.4
Outcome Measures Used in Cerebral Palsy
Participation
Participation for children with cerebral palsy is most often assessed with the Children’s Assessment of Participation and Enjoyment and the Preferences for Activities for Children. The Activities Scale for Kids and Assessment of Life Habits for Children are also employed in this domain. The Pediatric Evaluation of Disability Inventory and the Canadian Occupational Performance Measure assess both activity and participation realms. Some instruments address health status or quality of life, and may be placed in the domain of participation, while other instruments assess environmental factors. Common outcome measures in this group include the Child Health Questionnaire or other generic pediatric measures, the Cerebral Palsy Quality of Life Questionnaire for Children, and Goal Attainment Scaling.
Gross Motor Function Measure (GMFM)
The GMFM is a functional outcome tool that was developed specifically for use in cerebral palsy (215).
Widely used in research settings, the GMFM is also employed clinically for evaluation of children with cerebral palsy. The GMFM consists of a broad range of gross motor tasks, which a trained evaluator observes a child attempting to complete over a 45- to 60-min- ute time interval. Five dimensions of function (lying and rolling; sitting; crawling and kneeling; standing; and walking, running, and jumping) are examined. Specific scoring algorithms result in a score that can be used as an interval measure.Gait Analysis
Instrumented gait analysis is another objective functional measure that is widely used in cerebral palsy (216). Many centers do not use gait analysis; other centers rely upon it heavily, particularly in guiding treatment decisions such as orthopedic surgery. This technique can only be employed for children who have some ability to walk, even if they require gait aids. Gait analysis involves having a child walk in a specialized laboratory wearing markers and muscle activity sensors. Using sophisticated computers, cameras, and force plates implanted on the floor surface, the child’s movement patterns can be analyzed in great detail. Information about movement patterns in all planes, kinetics, and kinematics are generated. Although some controversy exists as to the reproducibility of gait analysis results and the means by which gait analysis should be employed to guide surgical decision-making (217), gait analysis remains a common tool for evaluation of cerebral palsy.