PARENTERAL FLUID THERAPY
Parenteral fluid therapy is the essential component of critical child care, required not only to correct dehydration but also to provide maintenance fluid/ electrolyte requirements in children who cannot be given oral fluids due to critical sickness, surgery, persistent vomiting or any other reason.
7.7.1 PRINCIPLES OF FLUID THERAPY
Some general principles for parenteral fluid therapy are as follows, while therapy in specific circumstances is discussed later.
Indications: Parenteral fluid therapy is mainly indicated in children with:
• Severe dehydration, hypotension or shock, when immediate volume replacement is life-saving,
• Persistent vomiting, with poor tolerance to oral feeds.
• Critical illnesses, e.g. coma, seizures, respiratory distress, etc. when oral feeding is not possible or contraindicated.
• Pre-and post-surgery fluid therapy.
• Systemic disorders, e.g. renal failure or CCF, which require fine-tuning of fluid and electrolyte intake.
Routes: Parenteral fluid therapy requires secure IV access with a peripheral venous line. In emergency, intraosseous infusion may be used temporarily for rapid fluid correction till IV access is secured (Ch 32.3).
Fluid volume requirements of each child vary according to their age, body weight, presence/severity of dehydration and primary disease, though approximate requirements may be calculated as sum-total of following:
• Maintenance requirements, essential for basal metabolism as well as to replenish normal fluid losses via urine, stools and insensible means, e.g. lungs and skin. Though dependent on metabolic rate (1 ml water for each caloric expenditure), maintenance fluid and electrolyte requirements may be practically calculated by actual body weight as per holiday and segar formula (Table 7.16). In smaller children (6-15 kg) maintenance volume must preferably be calculated with body surface area as 1400-1500 ml/m2.
Calculated fluid requirements must be increased by 20-30% in conditions with higher insensible losses, e.g. fever, hyperventilation, warmer care, etc.; and decreased by 20-30% in cases with oliguria or less insensible losses, e.g. hypothermia.
• Deficit requirements depend on the severity and type of dehydration (iso-/hypo-/hyper-natremic), though generally calculated as 10 ml/kg for each percent of expected weight loss due to dehydration, i.e. ~5%, 10% and 15% for mild/moderate/severe dehydration in infants and ~3%, 6% and 9% respectively in older children.
For example, if a 4 years child weighs 15 kg and has moderate dehydration, his/her weight loss is expected to be 6% and fluid deficit is expected to be 15 ? 6 ? 10 = 900 ml. Table 7.16 gives fluid and electrolyte requirements in dehydration of variable severity. Electrolyte requirements have been calculated assuming 60:40 fluid loss from ECF and ICF, as common in isotonic dehydration.
Concomitant fluid and electrolyte losses in stools, gastric aspirate, etc. need periodic assessment
TABLE 7.16: Fluid requirements in normal children
A. For maintenance:
Water:
(BWlt;10 kg) : 100 ml/kg
(BW 10-20 kg) : 1000 ml + 50 ml/kg for wt gt;10 kg
(BWgt;20 kg) : 1500 ml + 20 ml/kg for wt gt;20 kg
(max 2400 ml)
B. For deficit:
Water (10 ml/kg of expected wt loss[‡‡] [§§] * due to dehydration) Mild dehydration : 30 ml/kg (50 ml/kg in infants) Moderate dehydration : 60 ml/kg (100 ml/kg in infants) Severe dehydration : 90 ml/kg (150 ml/kg in infants)
C. Concomitant losses
*Expected wt loss is ~ 3% in mild, ~6% in moderate and ~9% in severe dehydration; (higher 5%, 10%, 15%, in infants).
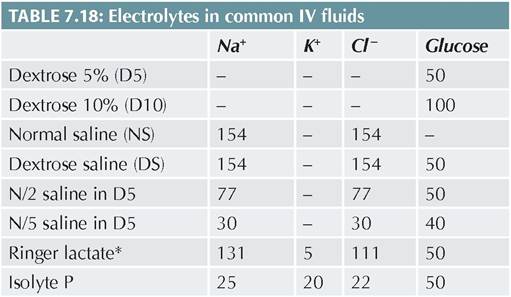
Na, K and Cl values in mEq/L, glucose in gm/L
*also contains lactate 29 mEq, which is in vivo metabolized into bicarbonate to prevent acidosis
TABLE 7.17: Composition of external abnormal fluid losses
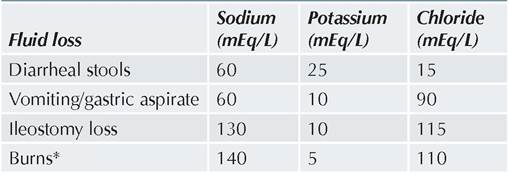
* and 3-5 gm/dl of protein
and replacement with suitable fluids.
Electrolyte requirements for this replacement depend on composition of body fluid/s, which are being lost (Table 7.17). About 10 ml/kg is considered as the concurrent loss for each large watery stool, and ~2 ml/kg for each vomiting.Choice of parenteral fluids depends on the estimated electrolyte requirements, need for nutrition (dextrose vs non-dextrose fluids) and primary disease. Various IV fluids with different electrolyte/dextrose concentrations are available commercially or can be prepared in hospital pharmacy under strict aseptic precautions (Table 7.18).
• For maintenance therapy, isotonic fluids, e.g. normal saline in DW 5% are recommended at present in all children except in neonates lt;28 days or those with cardiac/liver/renal disease, burns, malignancies or undergoing neurosurgery.
Earlier recommendations of maintenance fluid therapy with hypotonic N/2 or N/5 saline in Dextrose 5% are no longer valid due to risk of hyponatremia.
• For deficit correction, choice of fluid varies according to the route of fluid-loss, e.g. stools, gastric aspirate, etc. and laboratory electrolyte values. In general, Ringer lactate (Na+ 131 mEq/L) is preferred for this purpose in usual cases of diarrhea induced dehydration, with additional advantage of containing lactate that is converted into bicarbonate and prevents metabolic acidosis.
Monitoring: All cases on IV fluids should be monitored for changing needs of fluids/electrolytes, possibility of switch over to oral rehydration therapy and complications, e.g. overhydration, electrolyte disturbances, infection, thrombophlebitis or local extravasation.
7.7.2 FLUID THERAPY IN CLINICAL PRACTICE phase. By the end of this phase, child is expected to be circulatory stable.
Step II. Calculate 24-hour fluid requirements as sum total of maintenance + deficit needs, as discussed earlier.
Step III. Subtract the volume already infused in step I from this 24-hr fluid requirement calculated in step II and infuse remaining volume over next 24 hours using Isotonic saline in DW 5%.
Add 20 mEq/L of potassium in IV fluids after the urine output is established. In moderate to severe dehydration with fluid losses exceeding 5%, remaining volume should be infused more slowly over 48-72 hours, if switch-over to ORS is not possible.Concomitant losses via stools, vomitus or gastric aspirate, etc. must be added to the calculated volume. IV NaHCO3 (2-3 mEq/kg) may be added, if acidosis is suspected clinically but biochemical estimation is not possible.
Step IV. Gradual switch over to ORS, as soon oral feeds are acceptable.
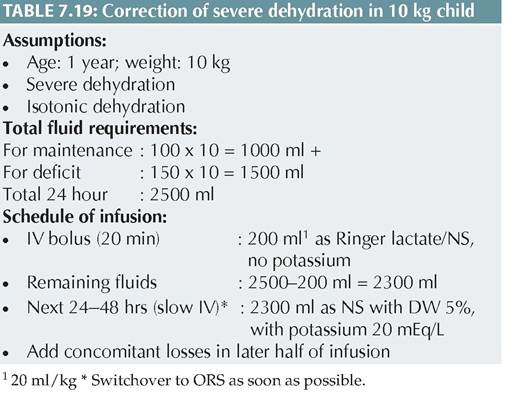
Table 7.19 provides a representative example for calculation of fluid requirements in a one-year old child, weighing 10 kg with severe isotonic dehydration.
Hyponatremic dehydration: While ECF losses are relatively higher in hyponatremic dehydration due to fluid movements from ECF to ICF, fluid therapy is similar to that for isotonic dehydration, except that calculated sodium deficit should be gradually corrected over first 12-24 hours, using high-sodium IV fluids, e.g. Ringer lactate or N/2 dextrose saline. Serum sodium correction should never exceed 10 mEq/L/24 hours. Only symptomatic hyponatremia with seizures is treated with 3% NaCl infusion at the rate of 1-2 ml/min (max 12 ml/kg) till seizures are controlled.
Hypernatremic dehydration: As ECF losses are comparatively less in hypernatremic dehydration due to osmotic withdrawal of fluids from ICF, only 3/4th fluid correction is required in these cases, using low-sodium
fluids, (e.g. N/2 dextrose saline). Sodium-free fluids should never be used in these cases due to risk of rapid drop in ECF sodium, osmotic fluid movement from ECF to ICF and cerebral edema. In any case, serum sodium fall should not exceed 8-12 mEq/L/24 hours.
7.7.3 FLUID THERAPY IN SPECIFIC SITUATIONS
General guidelines for fluid therapy in specific situations are discussed as follows:
Fluid therapy in diarrhea may be considered as prototype of fluid and electrolyte therapy in pediatric practice, as diarrhea is the commonest cause of dehydration in children.
Two methods of fluid therapy in diarrhea are in vogue—Standard fluid therapy, discussed earlier, and rapid rehydration method-later being more simple, practical and adequate in most cases.Traditional fluid therapy in diarrhea, requires complex calculation, which is neither practical nor necessary in most cases as: (a) prompt restoration of ECF will itself facilitate physiological corrective mechanisms, and (b) most cases tolerate ORS soon after initial correction and do not need prolonged IV therapy.
At the peripheral community level with limited resources, recent studies have proved safety and efficacy of simpler rapid rehydration in moderate to severe dehydration (WHO plan C, Ch 14.10).
This strategy involves a rapid infusion of Ringer lactate 30 ml/kg during first 30 min (1 hour in infants), followed by N/5 Dextrose saline ~ 70 ml/kg in next 2frac12; hours (5 hours in infants) and switch over to ORS, as soon as possible.
Fluid therapy in gastric losses: Loss of gastric juices is the major cause of dehydration in cases with persistent vomiting, e.g. congenital hypertrophic pyloric stenosis or in children requiring continuous nasogastric aspiration, e.g. intestinal obstruction. As gastric fluid contains relatively less sodium and more chlorides and potassium, hypokalemia and hypochloremic alkalosis are most important electrolyte disturbances in these cases. Fluid therapy in them is similar to traditional fluid therapy, except that:
• N/2 dextrose saline may be preferred for deficit correction in these cases.
• Potassium replacement should begin as soon as the child has passed urine.
• Hypochloremic alkalosis may be corrected by high- chloride IV fluids, e.g. isolyte G; or NH4Cl supplements after correction of hypokalemia.
Fluid therapy in critically sick children: Children with critical illnesses, e.g. acute neurological disorders (meningoencephalitis, head injury, hypoxic-ischemic injury, etc.), acute pulmonary disorders (pneumonia, asthma, respiratory failure) or those on ventilators, are likely to have fluid retention due to SIADH.
A simple and reliable indicator of this problem is the presence of hyponatremia despite concentrated urine with urinary sodium exceeding gt; 20 mEq/L. Important aspects of fluid therapy in these cases after initial fluid/electrolyte corrections, include:• Restriction of maintenance fluid volume to 2/3rd of calculated requirements; and
• Correction of hyponatremia: No correction is necessary for asymptomatic hyponatremia as fluid restriction itself allows a gradual recovery of serum sodium levels. However, cases with symptomatic or severe hyponatremia require slow correction with relatively hypertonic fluids, e.g. Ringer lactate, along with a diuretic, e.g. furosemide to enhance free water excretion. Rapid correction with 3% NaCl infusion (1 ml/min to max 12 ml/kg) is indicated only in cases with hyponatremic seizures.
Fluid therapy in surgery: Most common error during peri-operative fluid therapy is the overhydration, specially with plain dextrose fluids without electrolytes.
• Pre-operative fluid therapy in children for elective surgery aims to provide adequate carbohydrates for sustenance and maintenance requirements of fluids and electrolytes, which may be met with N/5 saline in dextrose 10%. However, children for emergency surgery need pre-operative fluid and electrolyte correction according to primary disease and laboratory investigations.
• During surgery, maintenance requirements should be given as isotonic normal saline or dextrose saline (without potassium), while surgical losses may be replaced with blood or plasma. As hyperkalemia is common during or immediately after surgery due to release of intracellular potassium after tissue trauma, potassium supplements should be avoided in this period.
• Post-operatively, SIADH is common and maintenance fluids should be restricted to 2/3rd of usual requirements during first 24 hours. Ringer lactate is the preferred fluid during this period. Potassium supplementation is indicated only after first 24 hours, unless warranted by laboratory reports.
Fluid therapy in malignancy: These cases, specially those beginning with induction therapy, are at risk of tumorlysis syndrome with hyperkalemia, hyperphosphatemia, hypocalcemia and hyperuricemia. Fluid therapy in these children should include additional maintenance fluids (usually 2-2.5 times) to ensure a urine output of 4ml/ kg/hour, using potassium-free fluids.
BIBLIOGRAPHY
1. Bagga A. Protocols in pediatric nephrology. CBS Publishers, New Delhi, 2019.
2. Feld LG et al. Clinical practice guideline: Maintenance intravenous fluids in children. Pediatrics 2018;142(6):e 20183083.
3. Reddi AS. Acid-base Disorders: Clinical evaluation and management. Springer Nature; Switzerland AG 2020.
More on the topic PARENTERAL FLUID THERAPY:
- Hypervitaminosis d
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Nausea and Vomiting
- 10.11 CHOLERA
- Ear Therapy
- Antiretroviral Therapy Today
- I URINARY TRACT INFECTIONS
- Haemorrhagic gastroenteritis in a dog
- Chapter 6 Complications of early pregnancy
- Chapter 29 Sexually Transmitted Diseases