PEDIATRIC BASIC LIFE SUPPORT
Primary aim of BLS is to restore and maintain vital functions till advanced life-support can be instituted, in order to preserve the organ viability and to help the return of spontaneous circulation (ROSC).
Evaluation and interventions in BLS are performed simultaneously in the following sequence : (a) assessment, (b) circulation,(c) airway, and (d) breathing.
Conventionally, BLS was a sequential actions to restore airway, breathing and circulation in that order, often termed as ABC of resuscitation. However, studies have shown that effort to restore the circulation by chest compressions must precede breathing support for better survival and outcome.
Accordingly, the approach has changed from ABC to CAB since 2015, i.e. circulation, airway and breathing, in that order. However, this change should not be construed as lesser importance to breathing support, which should begin within 20 seconds of initiation of the chest compressions. Important steps in BLS (Fig. 27.1) based on the current recommendations 2020, are as follows:
Step 1. Ensure safety of the patient and rescuer, as most of the emergency events requiring BLS happen out-of the hospital, e.g. on roads. Move the victim to a safer place if possible.
Step 2. Assess the response by gently tapping the child and asking a simple question, e.g. quot;Are you OK ?quot;. If the child is responsive, check for external injuries and need for medical assistance. Call for the help and alert the emergency response system without leaving the victim for long time. Do not move the child, if a spinal injury is suspected. Children with respiratory distress often assume a position that maintains airway patency and optimizes ventilation. Allow these cases to remain in a position that is most comfortable.
Step 3. Assess the breathing by looking at the victim.
• If breathing is normal, no resuscitation is required except close supervision till the help arrives.
Turn the child, if unconscious, in the recovery position (Fig. 27.2) to facilitate airway patency and decrease risk of aspiration. However, do not move the victims with suspected spinal injury.• If the child is non-responsive or not breathing (or only gasping), it should be assumed that cardiac arrest is present and resuscitation is required.
Step 4. Assess the pulse by palpating a peripheral pulse (brachial in infants, femoral/carotid in older children) for 10 seconds.

Fig. 27.1: Basic life support algorithm.
Based on AHA/AAP guidelines 2020.

Fig. 27.2: Recovery position.
• In absence of the pulse or pulse rate lt;60 minutes, begin chest compressions (Step 5), along with rescue breathing (step 6).
• In cases with pulse rate gt;60/min, begin rescue breathing @ 12-20 / minutes (Step 6). However, if pulse rate drops lt;60/minutes with signs of poor perfusion, begin chest compressions (Step 5).
Step 5. Chest compressions. High-quality chest compressions generate blood flow to vital organs. Chest compressions are indicated if pulse is absent or pulse rate is lt;60/minutes. Some important considerations during chest compressions are as follows:
• Place the child on a firm surface in supine position.
• Use Two-finger technique in infants, unless a second rescuer is present when Two-thumb chest encircling technique is preferable (Fig. 27.3).
• In older children, use the heel of one hand or two hands (Fig. 27.4) with two-hand technique being preferable due to less rescue fatigue.
• Compress the sternum ~2 fingers below the intermammary line in infants and over lower half of the sternum in older child. Xiphoid cartilage or ribs should never be compressed to avoid internal injury.
• Depth of compression is a major determinant of the efficacy of chest compressions and should be at least one-third of the anterior-posterior diameter of the chest, i.e.
~4 cm in infants and 5 cm in children.• Rate of the chest compression should be ~100-120/ minutes.
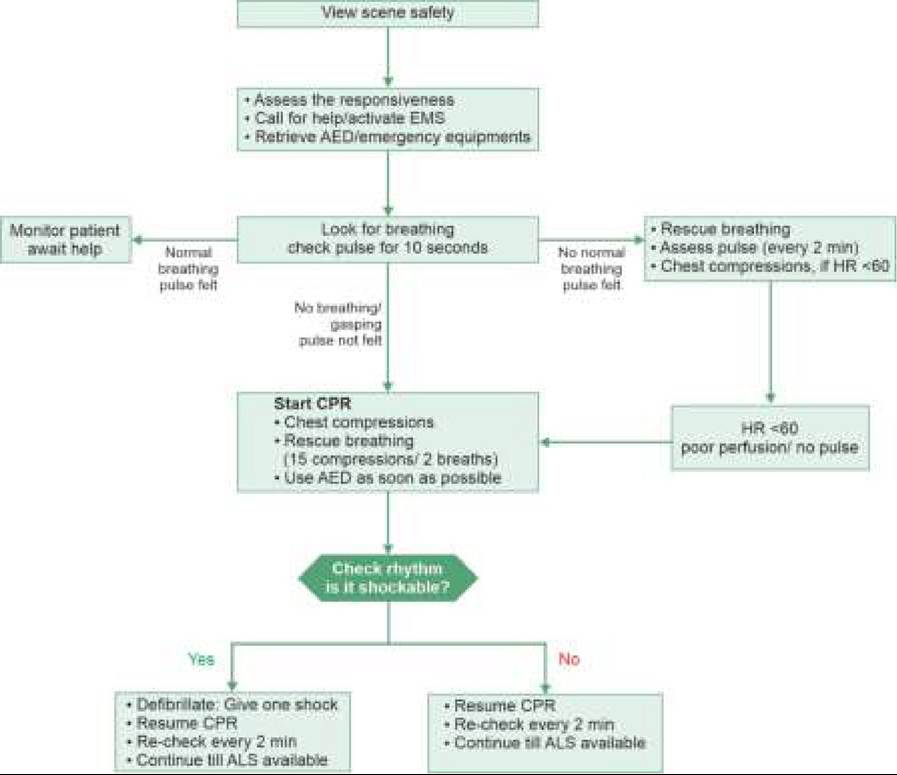
Fig. 27.3A and B: Chest compressions in infant: (A) Two-finger technique; (B) Two-thumb technique.

Fig. 27.5: Head tilt-Chin lift maneuver.

Fig. 27.4: Chest compressions in older child.
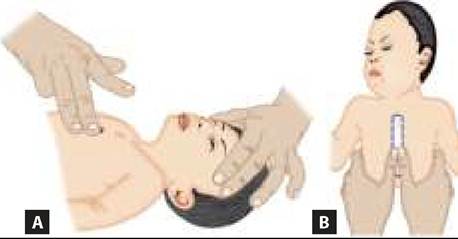
Fig. 27.6: Jaw-thrust maneuver.
• After each compression, chest should be allowed to recoil back to normal to allow adequate venous return, before next compression.
Step 6. Open the airway and ventilate. After 15 compressions, give two rescue breaths, after opening the airways.
Airway obstruction may be due to posterior displacement of tongue, mucus plug/ foreign body in airways or abnormal neck position. Head-tilt-Chin-lift maneuver (Fig. 27.5) is recommended or opening of the airways in both injured and uninjured victims. Use Jaw-thrust maneuver (Fig. 27.6) without head-tilt, if spinal cord injury is suspected. Gentle exploration of oral cavity to remove mucus plug or foreign body may be useful.
Rescue breathing aims to support ventilation, till mechanical help arrives. Some important considerations during rescue breathing are as follows:
• Use mouth-to-mouth and nose technique in infants and mouth-to-mouth technique in older children (Fig. 27.7).
• Ensure proper air-seal between rescuer's mouth and victim's mouth. Pinch the nose, if it could not be covered by rescuer's mouth.

Figs.
27.7A and B: Rescue breathing in: (A) Infant; (B) Child.• Each rescue-breath must last ~1 seconds. Slow delivery of rescue breath is important to prevent barotrauma and gastric distension.
• Pause after each breath and inhale deeply (rescuer), to maximize Oxygen concentration.
• Observe movement of the chest wall, during each rescue breath. Reposition the head, make a better seal, and try again, if chest does not rise adequately during rescue breath. Consider the possibility of foreign body if chest expansion is poor despite proper technique and repositioning.
Barrier devices to decrease the risk of infection during mouth-to-mouth breathing have not been found useful for this purpose and may increase the resistance to airflow.
Bag and mask ventilation is preferred over mouth-to mouth rescue breathing, if available, discussed in PALS section.
Step 7. Coordinate chest compressions and ventilations at the ratio of 15:2. However, such coordination is not necessary if an advanced airway is in place. In such cases, one rescuer continues to deliver at least 100 compressions/minute without pauses for ventilation, while another one delivers rescue breaths @ 8-10 breaths/min. Re-evaluate after every 2 minutes to decide about the need for further continuation.
Step 8. Defibrillation. Ventricular fibrillation can be the cause of sudden collapse, e.g. during sport events, or may develop during resuscitation attempts, presenting with pulse-less arrest. These cases need immediate defibrillation. If possible, all cases who do not respond to compression-ventilation cycles for 2 minutes must be assessed for need of Automated External Defibrillators (AED).
In cases with shockable rhythm, deliver a defibrillation dose of 2 J/kg, to be repeated as 4 J/kg if required. Coordinate chest compressions and shock delivery to minimize time-gap between compressions and shock and resume resuscitation, beginning with compressions, immediately after shock delivery.
In cases with non-shockable rhythm, continue compression-ventilation till help arrives.
Step 9. Activation of nearest emergency medical system. Nearby center, equipped with advanced life support facilities, should be alerted as soon as possible with complete details of—(a) location of emergency with contact telephone number, (b) actual event with expected number of casualties, (c) general condition of victim/s, to requisition help for BLS and transport, as well as to prepare them for emergency arrival.
CPR IN SPECIFIC SITUATIONS
Although abovementioned principles of CPR are applicable in most cases, following clinical situations warrant specific precautions, as follows:
Foreign body airway obstruction (FBAO) is a common emergency in pre-school children, to be suspected in any child with sudden respiratory distress, coughing, gagging, stridor or wheezing. Although removal of the foreign body may be life-saving in these cases, attempts should be made only if foreign body was witnessed or strongly suspected. For the purpose of resuscitation, FBAO is classified as mild, if victim can make a sound; or severe, if she/he cannot.
• In case, the foreign body is visible, remove it. However, Blindfinger sweeps should not be performed, as foreign body may be pushed back further into airway.
• In cases of mild FBAO, do not interfere and encourage spontaneous cough to clear the airway.
• In cases with severe FBAO, use Back-blows and chestthrust maneuver in infants and Heimlich maneuver in older children, discussed as below. Heimlich maneuver with abdominal thrusts is not recommended for infants, due to risk of abdominal injury.
Back-blows and chest-thrust maneuver is used in infants to expel unseen foreign body. Back blows are delivered by resting the child over rescuer's arm in prone, head-low position and giving five forceful blows between shoulder blades with heel of the hand. After careful turning-over the baby, Subsequent chest thrusts are delivered by placing him on rescuer 's thighs in supine, head-low position and giving five quick downward thrusts by two fingers over lower half of sternum.
These steps are repeated until foreign body is expelled or it becomes visible and can be removed by tongue-jaw lift maneuver. Else, rescue breathing should be given, before another attempt (Fig. 27.8).Heimlich maneuver is used in older children to expel unseen FB, by giving abdominal thrusts. In a conscious child, these thrusts are delivered in standing position, by encircling the child from behind placing thumb-side of one fist between navel and xiphoid process gt; grasping the fist with other hand to deliver a series of quick upward thrusts till foreign body is expelled becomes visible and may be removed by tongue-jaw lift maneuver. (Fig. 27.9). Else, rescue breathing should be given before another attempt In unconscious child, abdominal thrusts are delivered in supine position at the same site (Fig. 27.10).
Trauma: Important additional considerations during resuscitation of a trauma victim are as follows:
• Anticipate airway obstruction by dental fragments, debris, etc.
• Stop external bleeding with direct pressure.
• Minimize body movements in cases with suspected spinal injury and immobilize at least the torso on immobilization board, if possible.
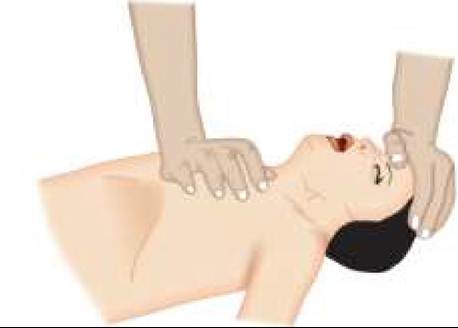
Fig. 27.8A and B: Back blow (A) and chest thrust (B) maneuver to relieve airway foreign body obstruction in infants.
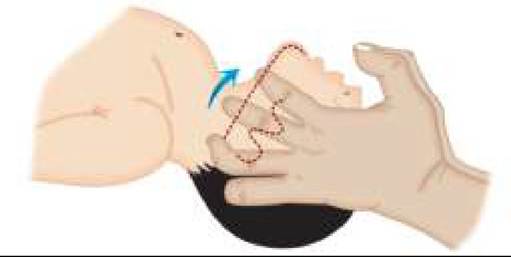
Fig. 27.9: Heimlich’s maneuver.
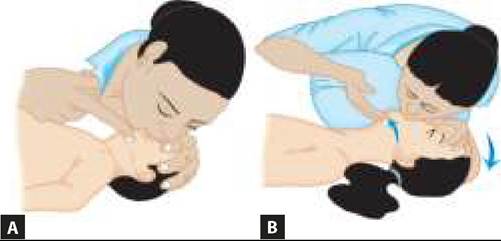
Fig. 27.10: Abdominal thursts for foreign body removal in lying down position in unconscious child.
• Don't use Head-lift-chin-tilt procedure in suspected cranio-cervical injury. Instead, Jaw-thrust maneuver may be used to open airways in these cases.
27.1.2