RESUSCITATION PROCEDURES AND DEVICE
Broad concepts of pediatric and neonatal resuscitation (PALS/NALS) have been covered in relevant chapters. This sections deals with common equipments and procedures used in resuscitation.
A. Suction devices may be broadly divided in three categories: (a) central suction system, desirable in intensive care units, (b) portable electric/foot-operated suction machine, commonly used in wards, and (c) oral (Delee's) mucus extractor. Important considerations during suction are:
• Suction catheter must be sterile/disposable, flexible and non-traumatic. A plain rubber catheter is preferred except to remove thick secretions or particulate matter by rigid catheter, e.g. nasogastric tube.
• Optimum suction force should not exceed ~80-120 mm Hg (~30 in newborns) to avoid mucosal trauma.
• Suction time at one attempt should not exceed 5 seconds to avoid prolonged hypoxia. If necessary, O2 supplement is necessary before next attempt.
• Heart rate should be monitored to detect significant bradycardia, due to vagal stimulation.
Important complications of suction procedure are: (a) mucosal trauma, (b) nosocomial infection and rarely, (c) sudden cardiorespiratory arrest due to vagal stimulation.
Delee's mucus extractor is a small, disposable, PVC suction device for neonatal resuscitation, with three parts:
(a) central bulb to retain aspirated mucus, connected to,
(b) a patient's end tube, and (c) a resuscitator's end tube with adopter (Fig. 32.9). As the resuscitator sucks from his/her end of tube, patient's mucus is collected in the bulb by negative pressure. Advantages: Delee's mucus extractor is the preferred suction device for intranatal or immediate postnatal resuscitation due to: (a) simple to use, (b) non-expensive, (c) disposable, (d) does not require electricity.
However, It is not effective beyond neonatal period, due to limited negative pressure, created by resuscitator's suction (lt;50-60 mm Hg).
Fig. 32.10: Oropharyngeal airway.
B. Oropharyngeal airway is a curved plastic/metal device of variable size (Fig. 32.10), used to prevent glossoptosis and provide clear airway/suction channel in unconscious children.
Appropriate size may be estimated by placing its flange at the corner of mouth, when the tip should reach the angle of mandible. It should not be used in a conscious/convulsing child to prevent tongue bite, due to risk of further trauma.
C. Oxygen delivery devices: Oxygen therapy aims to raise O2 content in inspired air (FiO2) in order to support blood oxygenation in hypoxic states and maintain PaO2 gt;60-70 mm Hg or SaO2 gt;95%. Common oxygen delivery devices may be broadly divided into three categories: (a) low-flow devices, e.g. direct nasal catheters/prongs or facemasks, (b) high-flow devices face-tents or oxygen-hoods, and (c) directed flow devices, e.g. bag/mask ventilation or endotracheal tube. Efficacy of these devices varies with O2 flow rate and mixing with expired/environmental air (Table 32.2). Some commonly used oxygen delivery devices are as follows (Fig. 32.11):
Nasal cannula is a simple low-flow oxygen delivery device, with two short plastic prongs fixed to a hollow face-piece. These prongs are inserted in anterior nares and O2 is delivered into nasopharynx. Though simple to use, nasal cannula is suitable only for children with
TABLE 32.2: Common oxygen delivery devices
*up to 60-70%, if tight-mask and reservoir is used
Fig. 32.11: Oyxgen delivery devices.
minimum oxygen requirements due to: (a) limited FiO2 delivery, i.e. 20-40% at flow-rate of ~4 L/min, and (b) variations due to nasal/oropharyngeal resistance and tidal volume.
Oxygen flow-rates of gt;4 L/min irritate nasopharynx without much improvement in oxygenation.Nasal catheter is a simple rubber catheter with multiple holes in distal 2 cm, which is lubricated and inserted into one nostril till it reaches nasopharynx. It has no advantage over nasal cannula with two major disadvantages: (a) local nasal trauma, and (b) gastric distension, if inadvertently placed in esophagus.
Face-mask consists of three parts: (i) rubber/PVC body, (ii) standard 15/22 mm connecting port, and (iii) faceseal. Two types of face-masks are available-round-rim face-seal and anatomical-shape face-seal. An ideal mask should be: (a) transparent to allow monitoring for cyanosis and vomiting, (b) non-traumatic with cushioned face-rim, (c) anatomically fitting to allow good air-seal, and (d) proper size to cover the nose and mouth but not the eyes.
A minimum flow-rate of 6 L/min should be used with face-masks to prevent re-breathing of expired CO2. A face mask delivers ~ 35-60% FiO2 at oxygen flow rate of 6-10 L/min. Many modifications, e.g. partial re-breathing mask, non-rebreathing masks and venturi-type masks are also used to deliver higher FiO2.
Uses: Apart from: (a) oxygen delivery, face masks are also used for, (b) bag and mask ventilation in emergency resuscitation, (c) aerosol therapy in young asthmatics via nebulizer or spacer/MDI.
Sterilization: Although pre-sterilized disposable masks are preferable, re-usable masks may be used after running-water wash, chemical sterilization and drying. Oxygen hood/tents are high-flow clear plastic shells that cover face (face tent/shield), head (oxygen hood) or upper part of body (oxygen tent), which deliver ~40-50% of FiO2 at the oxygen flow rate of 10-15 L/min. Although ~80-90% FiO2 may be delivered via well-fitted oxygen hood, these hoods are usually not enough for use in children beyond infancy.
D. Bag and mask ventilation is the simplest method for assisted ventilation in a child with inadequate ventilator efforts.
Indications: (a) intermittent positive pressure ventilation (IPPV) by face-mask or endotracheal tube, (b) continuous positive airway pressure ventilation or CPAP (connected with PEEP valve to maintain end-expiratory pressure of ~5-10 cm H2O).
Resuscitation bag: Although many types of resuscitation bags are available, most commonly used is AMBU bag (Ambulatory Manual Breathing Unit).
A resuscitation bag has following parts: (a) patient outlet, to which face mask is connected, (b) one-way fish valve to allow escape of expiratory air, (c) pressure-limited pop-off valve set at 35-45 cm H2O to prevent barotrauma,
(d) self-inflating rubber bag of variable sizes (250-750 ml),
(e) wide air-inlet on other end that may also be connected with oxygen reservoir, and (f) narrow oxygen inlet to connect with O2 source (Fig. 32.12).
Pnp-Bffvelw ?#8539;#947;q*rt
#8729;'. ' jiquot;1#915; w#8539; gt;IaI#8739;
Fig. 32.12: Resuscitation bag.
A self-inflating bag, not connected to oxygen source, delivers room air (~21% O2), while ~30-40% oxygen may be delivered after connecting it with oxygen inflow of 10 L/minutes. For higher oxygen concentrations (~90%), the air inlet should be connected with Oxygen reservoir or rebreathing-reservoir - a small bag or corrugated latex tube with open ends. In this setting, some oxygen in resuscitation bag enters the reservoir during each compression to enrich gaseous mixture for next breath. Complications: (a) barotraumas, e.g. pneumothorax, due to use of excessive pressure, (b) gastric distension, when used with face mask or misplaced endotracheal tube. Gastric distension may be minimized by inserting a nasogastric tube or Sellick maneuver (pressure on cricoid cartilage to occlude proximal esophagus).
Contraindications: Bag and mask ventilation is contraindicated in newborns with: (a) kerosene poisoning to avoid risk of aspiration, and (b) diaphragmatic hernia (intestinal distension may accentuate respiratory compromise).
However, they may be ventilated manually with resuscitation bag through endotracheal tube.Self-inflating bags with fish-mouth valve should not be used to provide supplement oxygen in babies with spontaneous efforts, as many of them cannot generate enough inspiratory efforts to open the valve.
E. Endotracheal intubation is the most effective method to ensure adequate airway and deliver 100% FiO2 via assisted manual or mechanical ventilation.
Indications: (a) Persistent airway obstruction, (b) poor response to bag-mask ventilation, (c) assisted mechanical ventilation during resuscitation, (d) endotracheal aspiration of mucus, meconium or foreign liquids, e.g. milk, (e) general inhalation anesthesia, (f) intratracheal instillation of drugs, e.g. surfactant in hyaline membrane disease or adrenaline during resuscitation.
Equipments required for ET intubation include laryngoscope and Endotracheal tubes (Fig. 32.13).
• Laryngoscope is a metallic equipment with two parts a handle with batteries and a blade with light source. Two types of blades are available - straight blade (Miller type) or curved blade (Macintosh type). Though the choice depends on personal experience, generally straight blade is preferred in infants and children
Fig. 32.13: Laryngoscope, blades and endotracheal tube.
lt;8 years due to relative anterior and cephalad location of larynx.
Both blades are available in four sizes (0-3)—Size 0 for preterms/low birth weights, 1 for neonates and infants, 2 for 2-10 years age-group and 3 for older cases. Postuse, laryngoscope should be cleaned by thorough washing under running water, followed by chemical sterilization or autoclaving.
• Endotracheal (ET) tube is a disposable, translucent portex tube, which may be plain or cuffed in the center. Cuffed tubes are self-retaining when inflated with air (not with water due to risk of aspiration) but rarely used in young children, as normal anatomically- narrow cricoid cartilage in them itself provides a functional cuff.
ET tubes are pre-sterilized by gamma radiation and disposable.ET tubes are available in various sizes or numbers, denoting internal diameter (2-16 mm). Generally 2.0-2.5 size is required in preterms, 3.0-3.5 in fullterms and 4.0-4.5 in infants. Beyond infancy, the required size may be calculated as age in years/4 + 4. As a thumb rule diameter of the ET tube should be equal to the diameter of patient's little finger.
Most ET tubes have a longitudinal radio-opaque line for X-ray confirmation of location and a transverse black line proximal to the tip, termed as vocal cord guide. Vocal cord guide should be at the level of vocal cords to ensure that the tip of the tube is above the bifurcation of trachea.
Procedure: Although ET intubation is an art, learned only by practice, important steps include:
Check the proper functioning of laryngoscope and select proper size of ET tube, gt; place the patient on a flat surface with head end near the edge, gt; position the head
with neck in semi-extended position to ensure proper alignment between mouth, pharynx and trachea gt; hold the laryngoscope with left hand and insert the blade into mouth in midline till it reaches the base of tongue and epiglottis is visualized gt; insert the endotracheal tube into glottic opening under laryngoscopic guidance gt; advance it till mid-trachea* gt; ensure the correct position**.
* Desired depth of ET insertion is calculated as - Age in years/2 + 12 in cm from alveolar margins).
** Position and patency of ET tube must be checked after insertion by: (a) observation of bilateral chest movements, (b) auscultation for bilateral air entry into chest, (c) auscultation for absent breath sounds over stomach, (d) check X-rays and (e) recording ETCO2 levels, if possible.
Complications of ET intubation include: (a) local trauma,
(b) sudden laryngospasm during attempted insertion, (c) hypoxia during intubation procedure*, (d) subsequent tube-block by secretions**, (e) unilateral lung collapse/ emphysema due to misplaced tube, and (f) nosocomial infection. ET intubation for prolonged period may cause—(a) dependence/ difficult weaning, and (b) late tracheal stenosis.
*IPPV with 100% oxygen via bag/mask should be given before and between the attempts of intubation, to prevent prolonged hypoxia. Each intubation attempt should not last for gt;30 seconds, before next IPPV. During procedure, baby should be monitored for bradycardia and color (cyanosis / pallor) to detect severe hypoxia. **Post-intubation, position and patency of tube should be checked periodically by abovementioned methods and repeated suction is frequently required to maintain tubal patency.
F. Tracheostomy is indicated in children with airway obstruction or difficult intubations, using a disposable tracheostomy tube (Fig. 32.14). It serves the same purpose as intubation, with an advantage of reducing dead space, but disadvantages of increasing the risk of infection, tracheal injury and sub-glottic stenosis. Procedural details of tracheostomy are beyond the scope of this book.
32
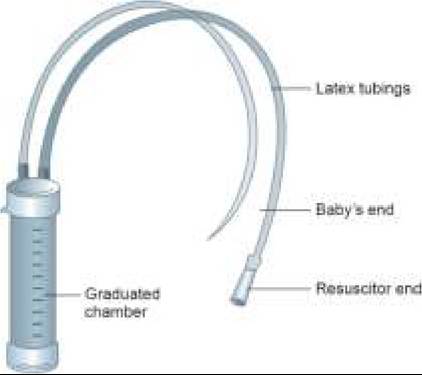
Fig. 32.14: Tracheostomy tube.
32.5