SAFE IMMUNIZATION PRACTICES
All injections involve breach in the continuity of skin hence, are potentially unsafe, according to a WHO report, ~30% of injections used for vaccinations worldwide are unsafe. A safe injection should not only harm the recipient, but also not expose the provider to avoidable risk or result in a waste that is dangerous to other people.
Important recommendations of safe injection practices are as follows:• Hand-washing: HCW should wash the hands with soap and water, if visibly dirty or may disinfect with an alcohol-based hand-rub between patients. Gloves are not necessary, though single-use gloves may be used and changed, if soiled. A HCW should avoid giving injections, if suffering from a local infection or cut which may come in contact with injected substance or blood or body fluids.
• Examine the vaccine product: Each vaccine vial must be examined for the name, expiry date and batch number, date of opening the multi-dose vial and status of vaccine vial monitor if present. Similar scrutiny is also necessary for diluents, if applicable.
• Prepare the vaccine: While many vaccines are currently available as single-dose pre-filled products, many others need to be drawn from multi-dose vials or reconstituted before use. Following precautions are necessary while preparing a vaccine for administration ± Vaccine shot must be prepared in a clean designated
area where blood or body fluid contamination is unlikely.
± All vaccines must be prepared fresh and should not be kept as pre-filled syringes in advance.
± Vials should be checked for cracks and leaks as well as any suspended particles in the contents before use.
± Swabbing the vial-top with antiseptic or disinfectant is not necessary though vials may be cleaned with a dry single-use antiseptic swab and not by stored wet-cotton balls.
Each vaccine must be reconstituted as per manufacturer 's recommendations, using only the diluents supplied by the manufacturer, if required.
Multi-dose vials carry higher risk of contamination and should be used strictly as per Open-vial Policy. Under Open-vial Policy, open multi-dose vials of some vaccines may be used in subsequent immunization sessions for up to maximum four weeks, provided: (a) expiry date has not passed, (b) vial was stored under appropriate cold-chain conditions, (c) vial septum is visibly clean and has not been submerged in water, (d) aseptic techniques were used to withdraw previous doses, and (e) vaccine vial monitor, if attached, has not reached the discard point.
- Needle used to withdraw the vaccine from this vial should not be left behind in the septum for redrawing, to avoid contamination.
- Whenever possible, vaccine shot must be prepared away from the sight of the child to avoid anxiety.
• Positioning the child: Unexpected motion at the time of injection may injure the child or cause needle-stick injuries to the HCW. Correct positioning with gentle restraining of the child is important to avoid such accidents.
- Child is usually more comfortable in presence of mother, who should be permitted to participate in positioning of the child to minimize the anxiety.
- Choice of the position depends on age of the child and site of administration, while Cuddling or lying- down position is preferred for infants, older children may be permitted to sit upright in mother's lap or held in the straddle position. School children may be immunized sitting upright independently, if cooperative (Fig. 9.6).
- Forcible restraining is not advisable, though a parent (or assistant) may tuck the child's legs between theirs to secure them or hold the child's free arm.
- Even though the child is securely positioned and restrained, she/he should be gently informed about the injection.
• Route of administration: Vaccines are usually administered via intramuscular, subcutaneous or intradermal route (Fig. 9.7) as per the manufacturer's instructions or national guidelines, which are not interchangeable and should be strictly followed.
- Intramuscular (IM) injections are given by piercing the skin at 90° with a longer 23-24 gauze needle. All vaccines, containing adjuvants are generally administered IM, due to higher risk of local reactions following superficial injections.
- Subcutaneous injections must be administered by pinching up the skin with provider's fingers and piercing it at 45-60 angle with a shorter 23-25 gauze needle.
- Intradermal injections, e.g. BCG, fIPV or ID-rabies are administered over left shoulder or upper arm using a tuberculin syringe and small 25 gauze needle, by stretching the skin between non-dominant thumb and fingers and piercing it at ~15 with the bevel of needle facing upwards. Only the needle tip should be introduced beneath the skin. A successful intradermal injection is reflected by formation of a small wheel at the site.
• Site of vaccination: NIS and other schedules generally specify the recommended site and side for each vaccine injection for the sake of uniformity, which should be adhered to unless the change is warranted due to local causes, e.g. infection, etc.
- IM injections in infants are usually preferred over anterolateral aspect of thigh (Fig. 9.8) due to inadequate muscle mass in upper arm. Older children may be given IM vaccines in deltoid region. No vaccine should be given on gluteal region as the antigen deposited in the fat may not invoke appropriate immune response.
- Subcutaneous injections are usually administered over outer aspect of the upper arm, though may be given over thighs in infants.
- Intradermal injections are given over the shoulder or upper arm, conventionally on left side.
- Two injections, when need to be given during same visit, must preferably be given on opposite sides. However, more injections can be administered on same site, separated by at least 2.5 cm to avoid overlap of local reactions.
• Use of sterile injection equipments: WHO no longer recommends the use of standard disposable syringes and needles due to risk of potential re-use.
Autodisable syringes are preferred for immunization purposes in NIS. Some important considerations while using selecting injection instrument are as follows:
Fig. 9.7: Correct techniques of intramuscular, subcutaneous and intradermal injections.
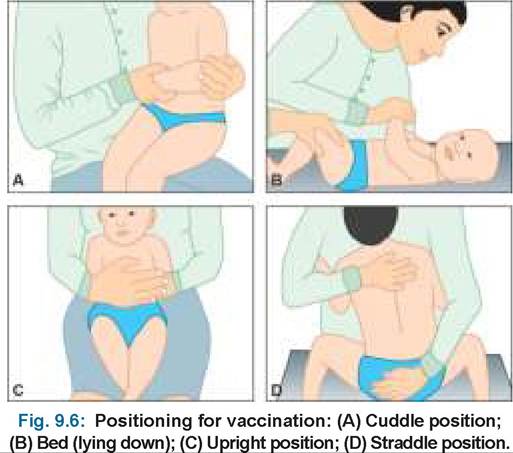
Fig. 9.9: Autodisable syringe.
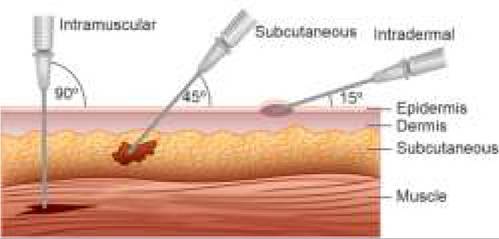
Fig. 9.8: Correct site of immunization in infants.
(A) Anterolateral aspect of thigh; (B) Upper arm (Deltoid region)
- Package containing syringe and/or needle should be carefully inspected before opening and discarded, if found to be punctured, torn or damaged.
- Changing needles between drawing vaccine into the syringe and injecting it into the child is not necessary, unless twisted or potentially contaminated.
- A longer 23-24 Gauze needle (min 2.5 cm in length) is preferred for IM injections to reach at deeper tissue plain while shorter needles may be used for SC or ID injections.
- While using an auto-disabled syringe (Fig. 9.9), plunger should not be pushed forward before the injection to inject the air in the vial, as it might disable it.
• Administering the injection: After the child is properly positioned and restrained and the injection is ready, following recommendations must be considered:
- Selected injection site should be inspected for any local infection, etc. and must be cleaned with a swab, if dirty. Cotton swabs stored wet in a multiuse container should not be used.
- Vigorous swabbing of the skin with antiseptic before injection is unnecessary and may add to the anxiety. Organisms colonizing the clean injection site are usually non-pathogenic. However, if an antiseptic swab is used, it should be prepared just before use and product-specific skin contact time must be adhered.
- No antiseptic swabs should be used for local cleaning before administration of live vaccines, e.g. BCG, which may deactivate pathogens.
- Aspiration, i.e. pulling back on the plunger after insertion of the needle but before pushing the liquid is not advised as no large vessels are present at the recommended sites and the process might be more painful for infants due to movement of needle.
• Waste disposal: Safe disposal of the injection waste is essential to prevent needle-stick injuries to HCW and re-use of contaminated injection equipments. Following recommendations must be considered for safe waste disposal:
- Needle should be cut at the point of use only with a electric or mechanical needle-cutter and disposed- off along with part of the syringe nozzle in the puncture-proof sharps container.
- Remaining part of plastic syringe and vaccine vial must be disposed in the red bag.
- Empty vaccine vials/ampoules and swabs, etc. may be discarded in yellow bags.
- Recapping of the used needle is a major cause of needle-stick injuries to the provider, and should be avoided. However, if necessary single-handed scooping-re-sheathing technique may be used to minimize the risk.
• Post-vaccination observation: All vaccinated cases must be observed for 15-30 minutes after injection for a major adverse event, e.g. anaphylaxis. All vaccination sites - fixed or outreach, must be equipped to handle anaphylaxis using anaphylaxis kits.
9.8.3