TUBERCULAR MENINGITIS
CNS involvement is the second most severe complication of tuberculosis after miliary tuberculosis, responsible for 60-70% of all TB-related deaths in children. Tuberculosis may involve any part of CNS, with wide spectrum of presentations (Table 18.29).
Tubercular meningitis (TBM) is the commonest manifestation of neurotuberculosis with high mortality and residual morbidity in survivors, discussed here.
Epidemiology: TBM is most common between 6 months - 3 years of age, with following risk factors—(i) BCG unimmunized child, (ii) low socioeconomic status, (iii) severe malnutrition, (iv) history of contact, (v) recent immunosuppressive illnesses, e.g. measles, pertussis, etc., and (vi) immunodeficiency states, e.g. HIV.
Pathogenesis: Tubercular infection of brain is usually caused by hematogenous spread from primary focus. Rarely, it may also reach from cervical lymph nodes via transcranial connecting lymphatics.
Hematogenous infection tends to be typically trapped in end-arteries to form a sub-meningeal cortical focus (Rich's focus), which may remain—(a) silent, (b) progress locally to form tuberculoma and present as a space occupying lesion, or (c) rupture over meninges to cause TBM.
TABLE 18.29: Types of neurotuberculosis
• Intracranial
- Tubercular meningitis
- Tubercular encephalopathy
- Tuberculoma
- Aseptic (Lincoln's) meningitis
• Spinal
- Arachnoiditis
- Tuberculoma
- Compressive myelopathy
- Polyneuropathy
Pathological characteristics in TBM include:
• Meningeal exudation due to intense inflammatory reaction, which is most prominent on base of the brain (basal exudates) and may lead to—(i) infranuclear cranial nerve palsies by entrapment of nerves, and/ or (ii) communicating hydrocephalus due to impairment of CSF absorption in arachnoid villi.
• Parenchymal Endarteritis obliterans, due to perivascular inflammation, leading to infarcts and focal signs.
• Choroidal tuberculoma and exudates, blocking CSF flow to cause obstructive hydrocephalus.
• Cerebral edema and impairment of blood-brain barrier, leading to altered sensorium, raised ICP and CSF abnormalities.
Clinical presentations are extremely variable, though a typical case presents with three stages:
1. Prodromal stage (stage of invasion) with insidious onset of fever, constitutional symptoms and signs of raised ICP, e.g. headache, vomiting, irritability and papilledema.
2. Stage of meningitis with—(a) signs of meningeal irritation, e.g. neck rigidity, Kernig's sign, etc.,
(b) seizures (c) focal neurodeficits, e.g. hemiplegia.
3. Stage of coma with—(a) loss of consciousness,
(b) decerebrate/decorticate posture (Fig. 18.11A) and
(c) altered vital functions, e.g. irregular respiration, hypo/hypertension, etc.
While each stage lasts for ~1-2 weeks, illness may progress rapidly without clear distinction of stages.
Atypical TBM may also present as: (a) pyrexia of unknown origin, (b) acute stroke, e.g. hemiplegia, (c) slowly progressive encephalopathy, (d) intracranial space occupying lesion, (e) recurrent seizures, (f) hysteria,
(g) hydrocephalus, or (h) isolated cranial nerve palsies.
Diagnosis of TBM is based on:
• Clinical indicators, e.g. (i) risk factors, (ii) history of contact, (iii) insidious clinical course;
• Supportive evidences, e.g. positive tuberculin test and/ or X-ray chest.
• CSF examination reveals straw-color CSF (Fig. 18.11B), cobweb formation, moderately raised proteins and
Fig. 18.11A: Tubercular meningitis: (A) Decerebrate posture.
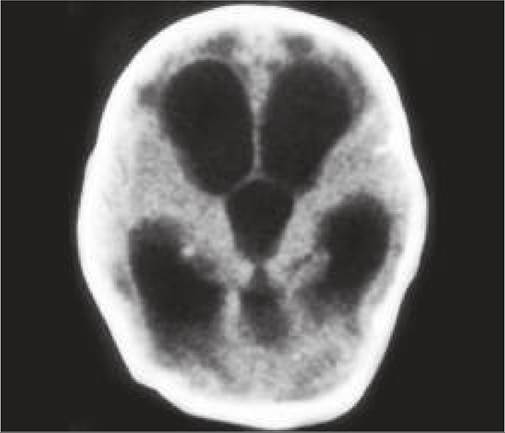
Fig. 18.11B: Tubercular meningitis:
(B) Straw-color CSF with Cobweb information.
cells (mainly lymphocytes) and mild hypoglycorrhachia (Table 18.6).
• Microbial confirmation from CSF with positive (i) AFB staining, (ii) microbial culture, (iii) molecular diagnosis, as discussed in Ch 10.13.
X-pert MTB-RMP (GeneXpert) not only to detect the organism but also the rifampicin sensitivity and results are available in 2 hours.• Neuroimaging with CT/MRI is highly informative, showing basal exudates, infarcts and hydrocephalus (Fig. 18.12).
Serological tests for TB antigen or antibodies or interferon assays have no place in diagnosis. However, elevated levels of adenosine deaminase and tuberculostearic acid in CSF-metabolites produced by degradation of lymphocytes and TB bacilli respectively, support the diagnosis of TBM.

Fig. 18.12A and B: Tubercular meningitis-CT scan showing: (A) Basal exudates with hydrocephalus; (B) Infarct.
D/D: TBM should be considered in d/d of any acquired CNS disease in endemic region. Common illnesses mimicking TBM include—(a) bacterial meningitis (Table 18.30), (b) encephalitis, (c) cerebral malaria, (d) enteric encephalopathy, and (e) intracranial space occupying lesions.
Management of TBM includes:
• Specific anti-tubercular therapy: As per NTEP recommendation for drug-sensitive neurotuberculosis, four drugs are used in intensive phase for 2 months followed by a continuation phase of 10 months with three drugs (2HRZE+10 HRE). While treatment of TBM should not be delayed for want to sensitivity results, it must be modified accordingly once the reports are available (Ch 10.13).
• Steroids, i.e. PO Prednisolone (1-2 mg/kg/d q6-8hr) for 6 weeks before gradual tapering are indicated in all cases to reduce inflammation and cerebral edema as well as to improve CSF penetration of drugs. Initially, IV steroids, e.g. hydrocortisone or dexamethasone may be used in acutely sick cases.
• Supportive therapy with:
- Nutrition and fluid/electrolyte maintenance.
- Constant monitoring and cardiorespiratory support
- Anti-edema measures, e.g. mannitol, hypertonic saline, acetazolamide, glycerol, etc. Steroids also act as anti-edema agents.
- Anticonvulsants, even in absence of seizures.
- Prophylactic antibiotics for initial 1-2 weeks, as it is often difficult to exclude pyogenic etiology.
- Physiotherapy, as soon as possible.
- Shunt surgery for hydrocephalus is commonly required in most cases of TBM.
Outcome of TBM depends on the clinical severity of disease on admission and appropriateness of treatment. Early diagnosed cases (stage I) have best prognosis with rare deaths and residual sequelae (lt;10%). Risk of mortality and residual lesions is high, i.e. 20-50% and 50-80% in stage II and III disease respectively.
Outcome is poor in cases with—(a) age lt;2 years, (b) severe malnutrition, (c) coma, seizures or focal signs
TABLE 18.30: D/D between BM and TBM

on admission (d) severe hydrocephalus and (e) poor therapeutic response in initial weeks.
Common sequelae of TBM are: (a) hydrocephalus, (b) secondary epilepsy, (c) focal motor deficits, e.g. hemiplegia, (d) mental retardation, (e) vision or hearing loss, (f) speech defects, and (g) endocrinal problems, e.g. obesity, diabetes insipidus, etc.
18.12.3