VACCINES IN NATIONAL IMMUNIZATION SCHEDULE
NIS in India include routine vaccination of all children with nine vaccines, i.e. BCG, HBV, OPV, IPV, DPT/Td, Hib, RV, PCV and MR, along with additional Japanese encephalitis (JE) vaccine in selected endemic districts.
Human papillomavirus vaccine (HPV) is likely to be introduced soon.BCG vaccine (bacille Calmette-Guerin vaccine) is the oldest amongst currently used vaccines (earliest vaccine was smallpox, used in 1798), named after its developing scientists - Leon Charles Albert Calmette and Camille Guerin (1921).
Contents: It is a live attenuated vaccine containing 0.1-0.4 million viable bacilli per dose. In India, Danish strain of Mycobaterium bovis is used to prepare BCG.
Supply and storage: BCG is supplied as a freeze-dried power in multi-dose, dark-colored vials (light sensitive) and should be reconstituted by mixing with diluents supplied with vaccine or sterile normal saline (not with distilled water, which is irritant) just before use. As it is extremely heat and light sensitive, reconstituted vaccine must be used within 3 hours.
Un-open ampoules should be stored in top-most compartment of refrigerator at 2-8°C.
Immunization schedule: BCG is given preferably at birth or the earliest possible opportunity within 48-72 hours of birth (not later than 7 days). Catch-up immunization is provided till 1 year in NIS, but recommended up to 5 years by WHO/IAP.
BCG vaccination is not advised in older children due to high likelihood of natural infection but may be given to older children if they are tuberculin-negative, on request.
Dose and administration: BCG is given intradermally over left shoulder as 0.05 ml at birth or 0.1 ml in older infants gt; 1 month of age. However, WHO recommends 0.05 ml till 1 years of age.
BCG is given with a tuberculin syringe and 26 gauge needle, after cleaning the site with sterile wet swab.
Spirit or alcohol swabs as should not be used as it may affect the viability of live vaccine bacilli. On correct administration, vaccine should raise a transient wheal of gt;5 mm over injection site. SC or IM injected vaccines are rapidly cleared by lymphatics and may not induce desired immune response or may cause local complications.After vaccination, the wheel disappears after 20-30 minutes and nothing is visible at site, followed by progressive induration after 3-4 weeks, ulceration after 6-8 weeks and scar formation after 10-12 weeks. In some children, the process of ulceration may be repeated 2-3 times, before eventual scarring.
Protective efficacy: Unlike other vaccines, BCG protects by inducing cell mediated immunity rather than humoral
some also containing IPV (Hexavalent).
immunity. Protective value of BCG is controversial, generally accepted as ~70-90% for severe disease, e.g. miliary or neurotuberculosis and 50-60% against pulmonary tuberculosis.
Successful uptake of BCG vaccine may be judged after 8-12 weeks, by local scar formation, tuberculin conversion or specific tests for cell mediated immunity. However, absence of scar does not necessarily mean absence of cell mediated immunity, which may disappear over time after 5-10 years. If a child fails to develop the scar after 12-16 weeks of vaccination, BCG may be repeated on the opposite side.
Side effects are rare and include:
• Local reactions including secondary infection or keloid formation are seen in 1:1000-10000 vaccinees despite correct administration, depending on strain and bacillary load in the vaccine. Danish strain used in India is more reactogenic.
• Regional lymphadenitis after ~4-8 weeks is not uncommon due to lymphatic spread of viable bacilli and no treatment is required except reassurance. It regresses spontaneously in next few weeks or months. However, suppurative lesions need antibiotics. Surgical drainage should be avoided to prevent sinus formation though very large nodes may be removed after completion of antibiotics, if required.
Antitubercular therapy is not required even if FNAC is positive for AFB, which is expected due to presence of bovine bacilli in the vaccine.• Disseminated disease (BCGiosis) is extremely rare (1:1-4 million) but may develop in immunocompromised children.
Contraindications are none, except congenital or acquired immunodeficiency states, e.g. AIDS and steroid/cytotoxic therapy. In asymptomatic HIV infected children, BCG vaccination is safe and should be given as a routine, unless they have evidence of severe immunosuppression.
DPT (Triple vaccine) is a combination vaccine against three diseases: Diphtheria, tetanus and pertussis. Depending on the pertussis fraction, this vaccine is termed as DTwP (containing whole cell killed bacilli) used in NIS; and DTaP (containing acellular pertussis antigens). DTaP is not provided in NIS. Another triple vaccine containing low-dose of diphtheria toxoid with acellular pertussis antigens (Tdap) is also available for use in older children gt; 7 years but not in NIS.
Other related vaccines without pertussis component include DT, Td (Low-dose diphtheria for use in older children #8805;10 years and mono-antigenic tetanus toxoid.
DTwP and DTaP vaccines are also available as combination vaccines with HBV and Hib (pentavalent),
Contents: DTwP contains diphtheria toxoid (25 Lf) tetanus toxoid (5 Lf) and killed whole cell pertussis bacilli (20,000 million).
Supply and storage: DTwP in NIS is administered as a pentavalent vaccine with HBV and Hib and should be stored in middle compartment of refrigerator (2-8°C).
Dosage and administration: 0.5 ml of vaccine is given IM over lateral aspect of thigh.
Immunization schedule: In NIS, Primary doses of DPT are given as pentavalent vaccine at 6th, 10 th and 14th week of life, followed by two boosters of stand-alone DPT at 15-18 months and 4-5 years.
Catch-up immunization below 7 years include three doses of DTwP at 0,1,6 months with a booster after
6 months of last dose.
Second booster is not required if the last primary dose was given after 4 years of age.DTwP/DTaP vaccines should not be used above
7 years of age for boosters or catch-up immunization (Low-dose diphtheria vaccines, e.g. Td/Tdap are used in them, if required).
Protective value is 100% for diphtheria and tetanus and ~80% for pertussis.
Side-effects are mainly due to pertussis fraction and include:
• Local reactions, e.g. pain, swelling and tenderness, which may be relieved with cold compresses.
• Transient fever for ~24 hours, which may be treated with paracetamol. Occasionally, it may lead to febrile seizures.
• Rare but serious neurological events, e.g. inconsolable cry, hypotonic-hyporesponsive episodes, seizures and encephalopathy.
Frequency of local reactions increases and systemic reactions decreases with increasing order of doses.
Inconsolable cry refers to gt;1 hour of continuous, inconsolable cry within 24 hours of vaccination. It occurs more frequently after the first dose and recurrence is unlikely after subsequent doses.
Hypotonic-hyporesponsive episodes (HHE) refers to sudden onset of limpness, reduced responsiveness and pallor or cyanosis within 48 hours of vaccination, (also reported with PCV vaccine). Recovery is spontaneous with no sequelae. Further doses may be given safely without recurrence.
Contraindications include:
• History of anaphylaxis or encephalopathy with previous dose.
• Progressive neurological disease
No pertussis-containing vaccines (not even DTaP) should be given as further dose in these cases (use DT). Cases with other neurological events may be given
further doses, if required, under caution and longer observation period, preferably in the hospital.
DTaP vaccines, instead of whole cell bacilli, contain two or more of the following five separately purified pertussis antigens—pertussis toxin (PT), filamentous hemagglutinin (FHA), pertactin (PRN), and fimbrial hemagglutinins 1,2 and 3 (FIM type 2 and 3).
It is also available in combination as pentavalent or hexavalent vaccine.Not used in NIS, DTaP can be used with similar dose schedule and have lower incidence of local pain and fever following vaccination. While DTwP vaccines are marginally more immunogenic, IAP recommends use of DTaP as a substitute of DTwP for primary as well as booster doses. DTaP may also be preferred to DTwP in children for booster doses due to lower reactogenicity and in those with history of severe adverse effects after previous dose of DTwP. It should be noted that serious side-effects, e.g. anaphylaxis and encephalopathy may develop even after DTaP, which should not be used for further doses after history of such events to previous dose of DTwP/DTaP.
Tdap vaccine, contains lower dose of diphtheria toxoid (2.5 Lf instead of 25 Lf). While not included in NIS, IAP recommends single dose of Tdap for:
• All fully immunized adolescents at 11-12 years,
• All pregnant women at 27-36 weeks irrespective of previous doses,
• Catch-up immunization in fully/partially unimmunized children older than 7 years as the first dose, followed by subsequent Td dose/s, if required.
Catch-up immunization is advised till 18 years and more than one dose of Tdap is not recommended except in pregnancy.
Td, a bivalent vaccine containing low dose of lower dose of diphtheria toxoid (Diphtheria toxoid 2 Lf) has replaced TT in NIS for (a) Booster doses in children at 10 and 16 years, and (b) Two doses 4 weeks apart in early pregnancy, (single dose, if last pregnancy dose received within 3 years)
IAP also recommends Td as: (a) subsequent dose for catch-up immunization after first dose as Tdap, (b) booster doses to fully immunized children every 10 years, and (c) instead of TT for wound care.
DT (Diphtheria toxoid 25 Lf, Tetanus toxoid 5 Lf), is no longer recommended except in rare instances when pertussis containing vaccine is contraindicated in children lt; 7 years.
TT (Tetanus toxoid 5 Lf) has been replaced by Td for all indications, except for wound care in some circumstances.
Polio vaccine: Two types of polio vaccines are available—a live, oral, Sabin vaccine (OPV) and an inactivated, parenteral Salk vaccine (IPV), named after their developers, each with its advantages and disadvantages.
After the elimination of poliomyelitis from the country, India is gradually and cautiously shifting from OPV to IPV to minimize the risk of vaccine-induced poliomyelitis, more common with OPV. However, only IPV schedule is not yet advisable due to risk of importing wild virus from endemic countries and OPV providing better local gut immunity than IPV.
Both OPV and IPV vaccines are used in NIS as well as in IAP recommended schedule, though with some differences.
Contents: OPV is a live attenuated, bivalent vaccine, containing only serotypes-I and III, while IPV is an inactivated trivalent vaccine containing serotypes I, II, III.
India has removed type II serotype from OPV since 2016, after it was declared eradicated globally in 2015. (Now type III has also been declared globally eradicated since 2019, and all cases of poliomyelitis at present are due to type I only).
Supply and storage: OPV is supplied as multi-dose vials with dropper. It is extremely heat-sensitive and maintenance of adequate cold chain is extremely vital. It should be stored at-20°C in large depots, in the freezer at clinic level and must reach immunization center at 2-8°C in vaccine carriers.
Each OPV vial is marked with vaccine vial monitor, i.e. a sticker with a lighter square inside a darker circle (see Fig 9.5). If the color of square is darker or matching the outer circle, vaccine is probably not potent and should not be used.
IPV is supplied as a multi-dose vial in NIS and as a single dose vial/prefilled syringe outside the program. Single dose IPV is usually in short supply as a standalone vaccine, but available as commercial combination vaccines with DTwP/DTaP + HBV and Hib vaccines. IPV should be stored in middle compartment of refrigerator at 2-8°C.
Dosage and administration: OPV is given as 2 drops orally while IPV is given either as: (a) Fractionated dose of 0.1 ml intradermally in NIS (fIPV), or (b) Regular dose of 0.5 ml IM/SC in private set-up (usually as combination vaccine).
Immunization schedule: In NIS, total five doses of OPV are recommended - at birth (zero dose), three primary doses at 6-10-14 weeks and a single booster at 16-24 months; along with three doses of fractionated IPV at 6, 14 weeks and 9 months. Additional OPV doses given during pulse polio campaign should not be counted in routine immunization.
IAP recommends only single dose (zero dose) of OPV at birth; followed by five doses of IPV including three primary doses at 6-10-14 weeks and two booster doses at 4-6 years.
Protective efficacy: OPV mainly provides local mucosal immunity by engaging receptor sites in the gut with
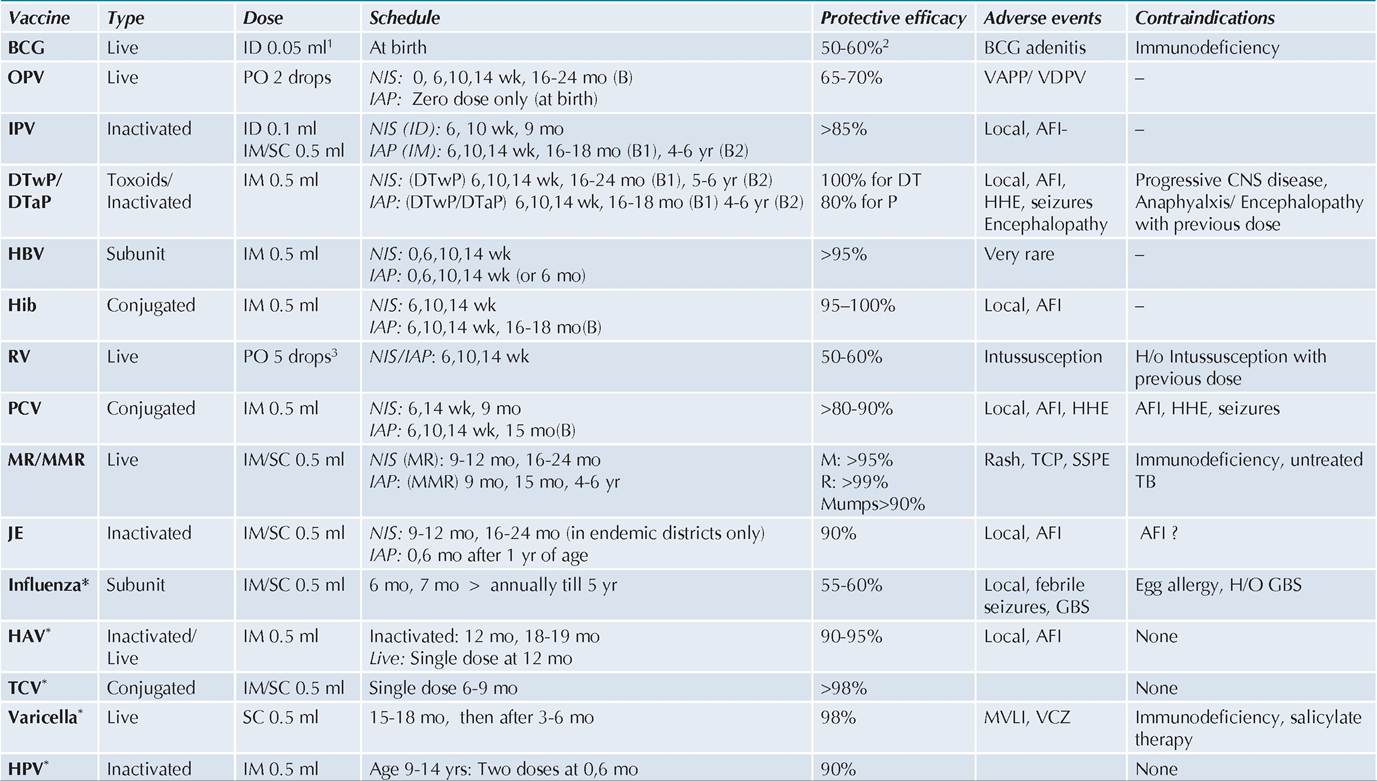
TABLE 9.2: Common Vaccines at a glance
Age gt;14 yrs: Three doses at 0,1/2, 6 mo
150 Textbook of Pediatrics
Starred (*) vaccines are not included in NIS at present.
Figures in parentheses after NIS/IAP denote total number of doses, required to complete immunization
10.1 ml after 1 mo of age, 2Over 80-90% for Neuro/Miliary TB, 3Doses of commercial preparations vary from 2.5-5 ml,
AFI: Acute febrile illness; B: Booster; GBS: Guillain-Barre syndrome; HHE: Hypotonic, Hyporesponsive episodes; MVLI: Modified varicella like illness; SSPE: Sub-acute sclerosing panencephalitis; TCP: Thrombocytopenia; VCZ: varicella zoster
vaccinia virus, thus preventing attachment of wild virus strains. While it is a highly potent live vaccine, both serotypes may not be taken up during each dose. Consequently, efficacy of the vaccine increases with increasing number of doses.
Protective efficacy of OPV is relatively less in developing counties like India (~65-70% after 3 doses) than in developed countries (~100%), perhaps due to interference with maternal antibodies and frequent presence of enteric infections preventing uptake of the vaccine.
OPV also provides herd immunity, even in unimmunized population due to excretion of vaccine virus in stools for variable period, which can infect the contacts to provide immunization.
IPV predominantly provides systemic immunity with seroconversion rate of gt;85% after three intramuscular doses. Fractionated interdermal doses are almost equally immunogenic at lower cost.
Side-effects: IPV is very safe except minor local reactions in some cases, while OPV carries potential but very rare risk of causing vaccine-related disease, as follows:
Vaccine associated paralytic polio (VAPP) is an extreme rare complication (1 per 2-4 million doses), more common with the first dose and in developed countries. In India, VAPP risk is lower, perhaps due to presence of maternal antibodies, birth dose of OPV and lower “takeupquot; of the vaccine. Defined as acute flaccid paralysis with residual weakness for 60 days after the onset with isolation of vaccine virus in stools (not wild virus), VAPP is caused by loss of attenuating mutations and reversion to neurovirulence during replication of the vaccine virus in the gut. VAPP may develop in the vaccine recipient (within 4-40 days of receiving OPV (recipient VAPP) or in contacts of the recipients, who is shedding of virus in stools (Contact VAPP).
Vaccine derived polioviruses (VDPV) denotes mutation of parent vaccine virus and recombination in the human gut with 1-15% divergence. These modified viruses are not only neurovirulent, but also transmissible and capable of causing outbreaks. VDPV are also classified as-cVDPV with evidence of virus circulation in the population, iVDPV in the immunodeficient person and aVDPV of ambiguous origin isolated from environmental sources without evidence of circulation. VDPV is more common following vaccination of immunodeficient children. Almost 90% of VDPV cases were due to Type II serotype, which has now been removed from the vaccine.
Possibility of VAPP/VDPV should be considered in any cases of acute flaccid paralysis with: (a) OPV vaccination in preceding 30 days, (b) contact with recently immunized child in preceding 60 days, or (c) pulse polio campaign in the community in preceding 60 days.
Contraindications are none, except for OPV in severe immunodeficiency states due to potential risk of VDPV in them or contacts. IPV may be safely used in these cases.
Measles containing vaccines (MCV) are combination vaccines including MR (Measles and Rubella) and MMR (Measles, Mumps and Rubella). Stand-alone measles vaccine has been withdrawn from India since 2018. Another combination vaccine of MMR with varicella (MMRV) is also available commercially. In NIS, only MR is used, though some states/cities provide one dose of MMR instead of second dose of MR at 16-24 months from their own resources.
Contents: All MCVs are live attenuated vaccines, containing Edmonston-Zagreb or Schwarz strain, containing of measles virus and Wister RA/3M strain of rubella virus (MR), with or without Urabe Am 9 strain of Mumps virus (in MMR).
Supply and storage: Both MR and MMR vaccines are available as single dose or multi-dose vial containing lyophilized powder along with diluent and should be reconstituted before injection.
All MCV Vaccines should be stored at 2-8°C and once reconstituted, should be used within 6 hour. Severe reactions, e.g. toxic-shock syndrome have been reported after delayed use of contaminated vaccine, which does not contain anti-bacterial preservative.
Dosage and administration: 0.5 ml IM or SC over anterolateral aspect of thigh for both MR and MMR vaccines.
Immunization schedule: IN NIS, two doses of MR vaccine are recommended at 9-12 months and 16-24 months, while IAP recommends use of MMR instead of MR with three doses at 9 months, 15 months and 4-6 years.
MCVs are not recommended before 9 months due to potential interference with maternal antibodies, though it may be given as early as 6 months during outbreaks. However any baby, who has received MCV before 9 months, should receive additional dose at 9 months to ensure adequate seroconversion. No boosters are needed, as single dose confers life-long immunity.
For catch-up immunization after 1 year of age, two doses of MMR are recommended with minimum four weeks interval. In adolescent girls, pregnancy should be excluded due to risk of congenital rubella syndrome.
Protective efficacy: Seroconversion rate for measles in 80-85% if given at 9 months and gt;95%, if given after 12 months of age. Seroconversion rate for rubella is even better gt;95% and gt;99% when given before or after 12 months respectively.
Almost all children vaccinated with MR after 12 months do not required second dose. However, high epidemiological risk of measles in infants aged 9-12 months in India has necessitated to provide MR vaccine as early as possible, i.e. at 9 months, followed by second dose after 12 months to ensure adequate protection.
Seroconversion rate for mumps-component following MMR vaccination is also good at ~90%, though antibody titers decline with time and third dose of MMR is recommended by IAP at 4-6 years to ensure by IAP, to ensure life-long protection against mumps.
Side effects: All MCVs are very safe, except mild local reactions, transient morbilliform rash after a week in 2-5% cases and transient thrombocytopenia as well as immunosuppression, which are often asymptomatic.
However, maximum number of immunization-related deaths are reported with MR/MMR due to inadequate aseptic precautions and bacterial contamination of the vial due to use beyond 4-6 hours.
Sub-acute sclerosing panencephalitis or SSPE (Ch 18.15) has been very rarely reported (lt; 1 per million doses) following MCV vaccinations.
Contraindications include (a) severe immunodeficiency states as these are live vaccines, (b) pregnancy due to potential risk of congenital rubella syndrome and (c) active untreated tuberculosis, as MCVs induce transient immunosuppression, which may fare-up the disease. MCV vaccinations should be deferred till antitubercular therapy has been given for 4-6 weeks.
Hepatitis B vaccine (HBV): Currently available HBV are recombinant vaccines, available as stand-alone vaccines or as combination vaccine with DPT, DPT+Hib, DPT+Hib+IPV or HAV.
Contents: HBV contains a suspension of alum-adsorbed recombinant HbsAg particles as 20 pg/ml.
Supply and storage: HBV is available as single or multi-dose ready-use vials with pediatric and adult dose formulations. In NIS, it is provided as pentavalent vaccine with DTwP and Hib.
Dosage and administration: HBV in children is given as 0.5 ml IM over anterolateral aspect of thigh. A higher dose of 1.0 ml is required for adults gt; 18 years of age.
Immunization schedule: In NIS, four doses of HBV are given, first dose within 24 hours of birth as stand-alone HbV (Birth dose) and subsequently 3 primary doses at 6-10-14 weeks as pentavalent vaccine with DTwP and Hib. IAP recommends similar schedule, but with last dose at 6 months of age rather than at 14 weeks.
Immunological response to HBV may be poor in preterms and LBW lt; 2000 gm, in whom the birth dose may be deferred till chronological age of one month (provided mother is HBsAg negative) or alternatively, the birth dose is given but not counted.
Infants born to HbsAg positive mothers should also receive HBIG (IM 0.5 ml) within 24 hours of birth along with HBV at a different site (Ch 15.4).
While three doses are enough to complete HBV immunization, birth dose is given additionally in routine immunization to ensure some protection to newborns of HBV positive mothers.
For catch-up immunization, only three dose schedule of HBV at 0, 1 and 6 months is recommended.
No booster is required, except in immunocompromised or occupationally exposed persons, in who antibody titers drop below the protective level over time (lt;10 mIU/ml) and booster dose may be needed after estimation of antibody titers.
Protective value: Seroconversion rate after 3 doses is gt;95%, with immunity lasing for gt;20 years. While antibody titers may decline with time, periodic testing is recommended only in children of HBsAg positive mothers, health workers and those with co-morbidities. Side-effects are very rare, except local pain/erythema and transient fever in some cases.
Contraindications are none, except in rare instances of serious allergic reactions to previous dose.
H. influenzae B (Hib) vaccine: Hib vaccine is available a stand-alone vaccine or as a combination vaccine with DPT, DPT+HBV, DPT+HBV+IPV, etc.
Contents: Hib vaccines are conjugated vaccines, containing a purified polysaccharide component of the organism, conjugated with a carrier protein to boost immunogenicity. Depending on the carrier protein, three Hib vaccines are available—HbOC (carrier mutant C. diphtheria toxin protein), PRP-T (carrier tetanus toxoid) and PRO-OMP (carrier N. meningitidis protein outer membrane protein complex), though last one is not available in India.
Supply and storage: Stand-alone Hib vaccines are lyophilized vaccines, supplied as single-dose (10 #956;g/ 0.5 ml) vials with diluent, to be reconstituted just before the use and should be stored at 2-8°C. However standalone Hib vaccines are not freely available in India at present and combination vaccines have to used.
Dosage and administration: 0.5 ml IM or SC, after reconstitution.
Immunization schedule for Hib varies with age, requiring three primary doses at 6, 10, 14 weeks followed by a booster at 12-18 months in infants lt;6 months, two primary doses at 0,1 month with a booster at 12-18 months in infants aged 6-12 months, and one primary dose and one booster after 8 weeks in children aged 12-15 months. Only single dose is required after 15 months of age, without any booster.
Vaccination beyond 5 years is not justified due to rarity of Hib infection, except in high-risk children, e.g. those with asplenia, splenectomy, sickle cell disease, etc. (Ch 9.4).
However in NIS, Hib is given as pentavalent vaccine at 6-10-14 weeks without any booster, while IAP schedule recommends one booster at 16-18 months, usually with DPT and IPV as combination vaccine.
Protective value: 95-100% for one year against culture proven invasive Hib disease. Hib vaccination also provides herd protection by reducing nasopharyngeal carriage of organisms.
Side effects are uncommon except mild fever and local reaction.
Contraindications: None, though dose should be deferred during acute severe febrile illness.
Rotavirus (RV) vaccine: Despite the high morbidity and availability of suitable vaccines, RV immunization was not widely used till recently due to potential fear of intussusception with older vaccines. With new generation RV vaccines, this risk has been minimized to acceptable limits and NIS has included RV in universal immunization program since 2016.
Contents: Currently, four RV vaccines are available in India-human monovalent vaccine (RV1), human-bovine pentavalent vaccine (RV5), human-bovine monovalent vaccine (RHBV1) and bovine-human reassortant pentavalent vaccine (BRV-PV). RHBV1 has been developed from a strain derived from Indian newborns and is being used in NIS, though all vaccines are equally effective and safe.
Supply and storage: RHBV1 and RV5 are liquid ready- to-use vaccine, while RV1 and BRV-PV are lyophilized vaccines to be reconstituted before use with given diluents. All RV vaccines must be stored at 2-8°C and not be frozen.
Dosage and administration: All RV vaccines are given orally but in different doses - 0.5 ml RHBV1, 1.0 ml RV1, 2 ml RV5 or 2.5 ml BRV-PV. However, in NIS, a different RHBV1 formulation is used, given as only 5 drops orally.
Immunization schedule in NIS, three doses of RHBV1 vaccine is given at 6,10 and 14 weeks with catch-up immunization at one month interval till 1 year of age (though 2nd#8725;3rd dose/s may be given later, if the first dose was given before 1 year of age). WHO recommends RV vaccination till 2 years of age.
IAP also supports similar schedule at 6-10-14 weeks (only two doses at monthly interval are required for RV1). However, it recommends that RV vaccination should be not be initiated after 15 weeks of age due to safety concerns and all doses should be completed by 32 weeks. Protective value: All RV vaccines are equally immunogenic and protective, with reported efficacy of ~50-60% against severe RV gastroenteritis (SRVGE), for at least two years. Protective efficacy is lower in developing countries than in developed countries (~80-90%), due to interference by maternal antibodies, widely prevalent malnutrition and co-infection with other enteric pathogens.
Side-effects are none except a definite but very small risk of acute intussusception (~1-2#8725;lac vaccines), specially after the first dose. However, benefits of vaccination to prevent SRVGE outweigh this miniscule risk.
Contraindications are none, except past history of intussusceptions. Vaccine can be co-administered with OPV.
Pneumococcal conjugate vaccine (PCV): Two types of pneumococcal vaccines are available—conjugate vaccine (PCV) for routine immunization and polysaccharide vaccine (PPSV), as an additional vaccine for high-risk children. PCV has been included in NIS since 2017. Following information pertains to PCV vaccines.
Contents: Currently three PCV vaccines are marketed in India, containing 10, 13 and 14 pneumococcal antigens. PCV10 is used in NIS. However, PCV with more than 14 serotypes are also in pipeline.
Supply and storage: All PCV vaccines are available as ready-to-use suspension in vials/prefilled syringes, which must be stored at 2-8°C and not be frozen.
Dosage and administration: 0.5 ml/dose IM for all vaccines.
Immunization schedule varies with age, requiring three primary doses at 6,10,14 weeks followed by a booster at 12-15 months in infants lt;6 months, two primary doses at 4 weeks interval with a booster in second year in infants aged 6-12 months, and two doses at 8 weeks interval after infancy. PCV13 needs only single dose after 2 years of age.
However in NIS, total three doses of PCV10 are given as two primary doses at 6 and 14 weeks and a booster at 9 months with catch-up immunization till 1 year of age.
IAP recommends total 4 doses for routine immunization at 6, 10, 14 weeks and booster at 12-15 months, with catchup immunization till 5 years of age, using manufacturers' recommended schedule.
PCV13 is also licensed for use as a single dose in older children 6-17 years and adults gt;50 years.
Protective value: All PCVs are equally immunogenic with gt;90% seroprotection following primary doses. However, protective efficacy depends on the number of serotypes included in the vaccine and number of doses. PCV 10 and 13 cover ~70% and ~80% of serotypes respectively, with protective efficacy of ~48%, ~87% and ~100% after 1, 2 or 3 doses respectively.
In general, protective efficacy of PCV is estimated to be ~80% against invasive pneumococcal disease due to vaccine serotypes and ~60% against all cases irrespective of serotypes, provided all primary doses are given before 6 months of age. Protective value is relatively less (~25-35%) against pneumococcal pneumonia or otitis media.
Side effects are rare and comparable with both vaccines, except local reactions and mild fever. Hypersensitivity,
seizures and hypotonic-hyporesponsive episodes have been rarely reported.
Despite excellent efficacy of PCV vaccines, a major concern is the Serotype replacement disease, i.e. causation of disease due to serotypes not including in the vaccine, thus offsetting the benefits of immunization. Surveillance programs have documented this phenomena in countries with high immunization coverage, despite substantial reduction in invasive pneumococcal disease.
Contraindications are none except severe allergy to previous dose or carrier protein, e.g. diphtheria toxoid.
Pneumococcal polysaccharide vaccine (PPSV) is an unconjugated polysaccharide vaccine containing 23 serotypes, responsible for gt;80% cases of serious disease. However, it is poorly immunogenic in children lt;2 years and does not reduce nasopharyngeal carrier state. It is given as single dose (0.5 ml SC/IM), only to high-risk children, i.e. those with chronic lung/heart disease, CSF leakage, cochlear implant, anatomical/functional asplenia, sickle cell disease and immunodeficiency. Revaccination is required after 3 years, but more than two doses are not recommended due to immunological hyporesponsiveness.
IAP does not recommend use of PPSV alone in these cases, who should receive PPSV only after completing age-related PCV immunization, at least 8 weeks after the last PCV dose. High-risk children, even if already vaccinated with PPSV, should receive recommended PCV doses.
Japanese encephalitis vaccine: Government of India has identified ~268 endemic districts for JE, where this vaccine is included in NIS. IAP recommends it only to— (a) children residing in endemic regions and (b) travellers to these regions, staying for gt;4 weeks.
Contents: Currently, three JE vaccines are licensed in India—one live attenuated vaccine derived from SA14-14- 2 strain and two inactivated vero-cell derived vaccines from different strains, i.e. SA14-14-2 strain and 825146XY strain from Kolar, India. Of these, only live attenuated vaccine is used in NIS, though others are commercially available.
Supply and storage: Live JE vaccine is a lyophilized vaccine, to be reconstituted before use. Both inactivated vaccines are liquid suspensions. All vaccines must be stored at 2-8°C, though live vaccine is heat-stable at 37°C for 7-10 days.
Dosage and administration: Live vaccine is given as 0.5 ml SC over left upper arm (Right upper arm is used for MR vaccination during same visit), while inactivated vaccines are given as 0.5 ml IM (0.25 ml for SA14-14-2 vaccine in children lt;3 years).
Immunization schedule: under NIS, two doses of live JE vaccine are given at 9-12 months and 16-24 months, with catch-up immunization till 15 years of age (or even more in some states).
IAP recommends two doses of inactivated vaccines at one month interval after one year of age with catch-up immunization till 18 years of age.
Protective efficacy: Efficacy of live vaccine is ~90% with two doses and gt; 90% with both inactivated vaccines, though titers may decline gradually.
Side effects: All JE vaccines are equally safe except transient fever and local reactions in few cases.
Contraindications are none, though vaccination should be avoided during acute febrile illness.
9.2.2