VITAMIN A DEFICIENCY
Vitamin A deficiency, till recently, was the commonest cause of preventable blindness in Indian children. While the prevalence of severe disease has substantially declined in recent years due to preventive programs, subclinical deficiency continues to be common with a prevalence of ~1-3% in preschool children.
Physiology: Vitamin A is a fat-soluble vitamin (Table 6.12), existing in two forms:
a. Pre-formed vitamin, e.g. retinol, present in animal sources; and
b. Pro-vitamin, e.g. ^-carotene, present in plant sources, which is converted to retinol in the gut.
Retinol is actively accumulated in liver (as retinyl palmitate) during last trimester of pregnancy and breastfeeding. Postnatally, retinol is better absorbed than #946;-carotene and transported in blood, bound to a retinol- binding protein.
RDA for vitamin A in children is ~350-600 #956;g#8725; day increasing with age to ~800-1000 #956;g#8725; day in adolescents, all values in terms of retinal equivalent (1 RE = 3.3 IU)
Dietary sources: Important source of vitamin A include yellow fruits, milk and animal products and fortified foods and at least half of the RDA should be derived from animal sources.
TABLE 6.12: Vitamin A at a glance
RDA: 350-1000 #956;g RE (1200-3000 IU)
Dietary sources
• Plant foods:
Yellow fruits: Mango (1000 IU), papaya (400 IU)
Vegetables: Carrot (4000 IU), spinach, amaranth
• Animal foods:
Milk products: Butter, margarine, cheese
Non-veg: Eggs, liver, fish, cod liver oil (54,000 IU)
• Fortified foods: Vansapati ghee
Functions
- Production of rhodpsin—night-vision pigment
- Maintenance of epithelial integrity
- Anti-oxidant (free-radical scavanger)
- Others - in bone metabolism, spermatogenesis, etc.
Deficiency states
• Xerophthalmia
• Phyrnoderma (follicular hyperkeratosis)
• Susceptibility to infections
Toxic effects (hypervitaminosis)
• Acute: Pseudotumor cerebri
• Chronic: Dry skin, alopecia, hyperostosis (limb-pains)
• Carotenemia: Yellow discoloration of skin
RE: Retinol equivalents (1 #956;g = 3,3 IU)
Functions: Vitamin A is essential for retinal functions, maintenance of epithelial integrity to resist infections and removal of toxic free-radicals from body.
Vitamin A Deficiency (VAD)
Etiology: VAD is most common in toddlers and preschool children from low socioeconomic status. Common causes of VAD include:
a. Dietary deficiency
b. Malabsorptive states, e.g. chronic diarrhea, worm infestations, etc.
c. Impaired metabolism, e.g. in chronic liver disease
d. Reduced transport proteins, e.g. in malnutrition, nephrotic syndrome, etc.
e. Higher requirements in infections, e.g. measles.
f. Less intrauterine stores, e.g. in preterms
g. Darrier disease—a genetic defect (vitamin Adependency). Clinical manifestations of VAD may be divided into two broad groups—ophthalmic (xerophthalmia) and extra-ophthalmic manifestations.
A. Xerophthalmia denotes a spectrum of ocular signs in VAD (Table 6.13) including:
• Night blindness, i.e. inability to see clearly in dim-light or slower dark-adaptation.
• Conjunktival xerosis, i.e. dry, wrinkled, lusterless, muddy conjunktiva due to cornified epithelium and
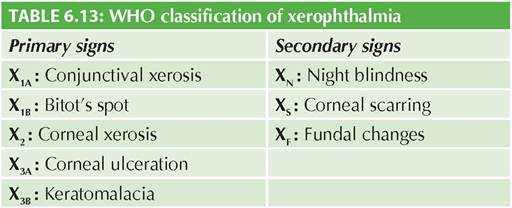

Fig. 6.7: (A) Bitot's spot; (B) Keratomalacia.
Bitot' spots—chalky gray triangular plaques, generally near the temporal limbus, due to heaped-up dry epithelium (Fig. 6.7A).
• Corneal lesions of variable severity: (i) xerosis, i.e. dull, dry and cloudy cornea, (ii) ulcers, limited to a few layers of cornea, or (iii) keratomalacia, i.e. liquefaction and rupture of full-depth cornea, leading to loss of vision (Fig. 6.7B). Even mild cases may lead to corneal scarring on recovery.
• Fundal changes, e.g. retinal xerosis and detachment.
B. Extra-ocular manifestations include:
• Phrynoderma (follicular hyperkeratosis), presenting as dry and scaly skin with toad-like texture, specially over extensor aspects of extremities, e.g. dorsum of tibia, knees and elbows. Phrynoderma is also associated with essential fatty acid deficiency.
• Recurrent respiratory infections, due to squamous metaplasia of respiratory mucosa.
• Recurrent urinary tract infections, pancreatitis or parotitis due to epithelial metaplasia of urinary or exocrine tracts.
• Rarely, atrophy of genital epithelium may lead to reproductive dysfunction in adults.
Diagnosis of VAD is largely clinical, though subclinical deficiency may be identified by:
a. Conjunctival impression cytology (CIC), to detect loss of mucus-secreting goblet cells and epithelial metaplasia on special staining,
b. Dark-adaptation test, and
c. Low plasma carotene levels (lt;20 #956;g#8725;L).
Treatment: As per WHO recommendation, standard treatment of VAD includes 3 age-dependent doses of
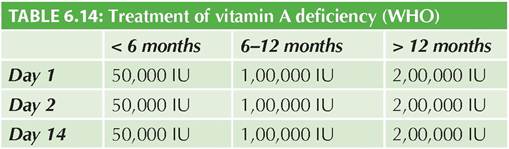
concentrated, preferably fat-soluble vitamin A (1,00,000 IU#8725;ml), given orally, on day 1, 2 and 14 (Table 6.14).
In cases with malabsorption or persistent vomiting, IM therapy with water soluble vitamin A (50,000 IU#8725;ml) may be used, given as half of the oral dose with same schedule. Local ophthalmic treatment of corneal lesions with antibiotics, mydriatics and eye-padding is equally important.
All cases treated for VAD should receive dietary counseling and vitamin A prophylaxis till 6-8 years of age (2,00,0000 IU every 6 month) to prevent the recurrence. Prevention of VAD includes nutritional counseling, vitamin A supplementation, fortification of dietary feeds (see national program below) and prevention of precipitating illnesses, e.g. measles.
National Control Programme Against Nutritional Blindness Due to Vitamin A Deficiency
Launched in 1970, currently this program is a component of National Health Mission, aimed to decrease the incidence of VAD and consequently preventable blindness. Prevalence of night blindness in pre-school children is considered as the best indicator of VAD, classified as severe (gt;5%), moderate (1-5%) and mild (lt;1%).
Beneficiary: Children from 9 months to 5 years.
Components of this program include:
• Universal prophylaxis with 6-monthly administration of oral vitamin A 1,00,000 IU (lt;1 year) and 2,00,000 IU in older children, from 6 months to 5 years of age. This protocol was first developed by National Institute of Nutrition, Hyderabad and later adopted by WHO as global strategy. Presently, first two doses are given during immunization visit at 9 months (with MR vaccine) and 15-18 months (with first booster dose). Subsequent doses at 24, 30, 36, 42, 48, 54 and 60 months of age are given in some states. IAP recommends this vitamin A administration to all children only till 3 years of age.
• Additional doses of vitamin A, after illnesses, e.g. measles, severe PEM, chronic diarrhea and long febrile illnesses.
• Dietary counseling, to encourage consumption of cheap and locally available vitamin A rich foods.
• Prevention of precipitating illnesses, e.g. measles by vaccination coverage and breastfeeding promotion.
• Periodic monitoring and evaluation.
Note: In national program, oral vitamin A is supplied as multi-dose liquid preparation (1 lac IU#8725;ml), with a special 2 ml spoon. Only this spoon should be used and not the regular 5 ml spoon to avoid over-dosage.
Hypervitaminosis A
Being fat-soluble, excess vitamin A is not readily excreted in urine and accumulates in tissues with following presentations:
• Acute hypervitaminosis, due to acute preventive or therapeutic overdose (gt;3,00,000 IU), presents as pseudotumor cerebri, i.e. transient, self-limiting, benign intracranial hypertension with headache, vomiting, drowsiness, bulging fontanels and/or papilledema (Ch 18.4). Exact mechanism is unknown, probably relates to massive rupture of lysosomal membranes.
• Chronic hypervitaminosis due to prolonged vitamin A therapy, e.g. for acne, presents with anorexia, weight loss, dry pruritic skin, alopecia, tender extremities (hyperostosis on X-ray), hepatosplenomegaly and pseudotumor cerebri.
• Hypercarotenemia, asymptomatic, transient yellowish discoloration of skin/body fluids, due to excess consumption of #946;-carotene containing fruits.
Massive vitamin A administration in first trimester may also have severe teratogenic effects on fetus.
6.3