VITAMIN D DEFICIENCY RICKETS
Vitamin D deficiency is estimated to be present in ~22-90% of infants and ~ 14-24% on older children and adolescents, though many cases are subclinical. Rickets is the commonest manifestation of vitamin D deficiency in children, characterized by failure of mineralization of the growing bones, which should not be confused with osteomalacia, i.e.
defective mineralization of mature bones, or osteoporosis, i.e. demineralization of premineralized bones.Rickets may be broadly divided into two categories:
(a) Vitamin D deficiency or nutritional rickets, and
(b) Vitamin D-resistant or dependent rickets (Table 6.18). Nutritional rickets accounts for over 90% cases in childhood, discussed in this section.
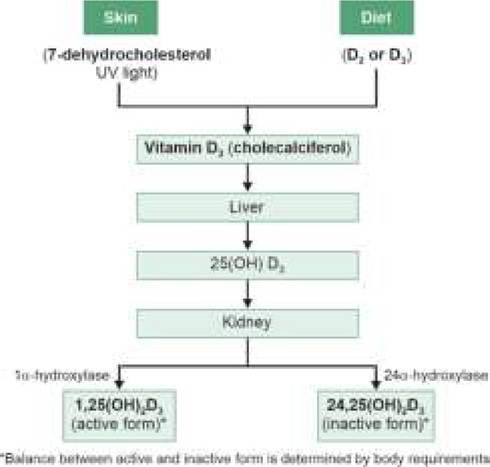
Fig. 6.9: Vitamin D metabolism.
TABLE 6.18: Etiological classification of rickets
A. Vitamin D deficiency (nutritional) rickets:
- Higher requirements in growing child
- Inadequate dietary intake
- Lack of exposure to sunlight
- Poor stores at birth—preterms, IUGR
- Malabsorption states
- Anticonvulsant therapy
B. Vitamin D resistant (refractory) rickets:
- Chronic hepatic disease
- Chronic renal disease (renal osteodystrophy)
- Hypophosphatemic rickets
#9830; Familial hypophosphatemia
#9830; Renal tubular acidosis or Fanconi syndrome
C. Vitamin D dependent rickets
- Type 1: Autosomal 1-hydroxylase deficiency
- Type 2: End-organ resistance to vitamin D
Etiologically, Vitamin D deficiency is rarely dietary, mainly seen in rapidly-growing children due to relatively higher requirements.
Inadequate endogenous synthesis due to limited sunexposure in dark-skinned population, high altitudes or veil-wearing communities, e.g. muslins, is another contributory factor for rickets in India, as also poor maternal stores in vitamin D deficient mothers.
Malabsorption states, chronic liver disease and chronic renal diseases also impair vitamin D metabolism, leading to vitamin D deficiency.
Pathophysiology: Vitamin D deficiency leads to reduced calcium and phosphorus absorption from gut and reabsorption from kidneys with consequent rise in PTH levels to maintain normocalcemia. High PTH activity stimulates calcium mobilization from bones leading to:
• Deficient mineralization of growing osteoid tissue with typical clinico-radiological changes in rickets;
• Increased osteoblastic activity with elevated serum alkaline phosphate levels-first biochemical change in rickets.
Increased renal reabsorption of calcium leads to compensatory phosphorus excretion and low serum phosphorus levels-second biochemical change. Normocalcemia is usually maintained in rickets by elevated PTH levels, except in severe cases.
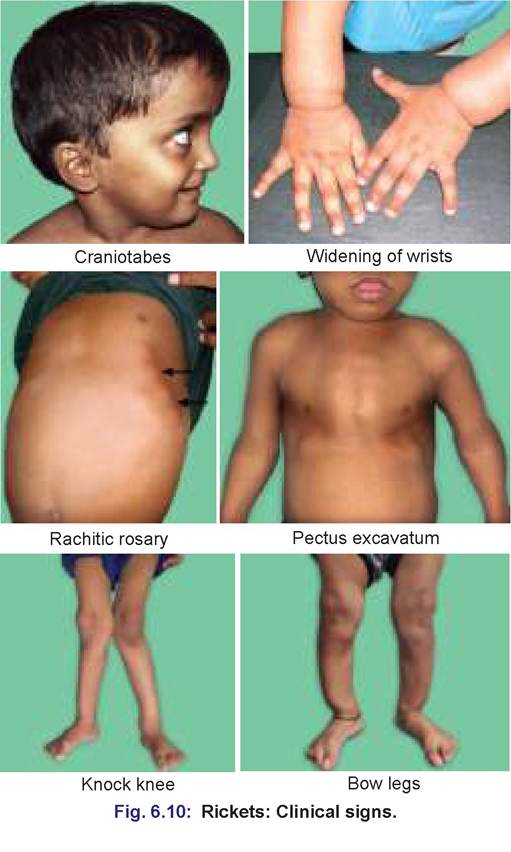
Clinical manifestations: Rickets commonly present at 6 months-2 years of age with bony deformities and hypotonia of supporting ligaments/muscles. Important clinical features of rickets include (Fig. 6.10):
• Craniofacial changes:
- Craniotabes—softening and thinning of skull bones with ping-pong ball like resilience on pressure over parietal bones, which is normal up to 3 months of age;
- Frontal bossing—prominence of frontal bones;
- Caput quadratum—box-head or hot cross-bun appearance due to fronto-parietal bossing;
- Delayed closure of anterior fontanel;
- Delayed dentition.
• Thoracic changes:
- Rachitic rosary—round, non-tender beading due to widening of costochondral junktions;
- Harrison sulcus—a groove/depression along the lower costal margins
- Sternal deformities like pectus excavatum, i.e. depression of sternum, pectus carinatum, i.e. forward projection of sternum, or pigeon-chest deformity;
• Limb deformities:
- Widening of wrist/ankles (double malleolus) due to widened epiphysis and metaphysic;
- Gait abnormalities, e.g.
knock-knee (genu recur- vatum), bow-legs and coxa-vara;- Green-stick pathological fractures of long bones.
• Spinal deformities:
- Kyphosis or scoliosis due to lax ligaments;
- Short stature due to deformed spinal curvature;
• Generalized hypotonia with:
- Pot-belly, due to abdominal muscle hypotonia;
- Visceroptosis due to ligamental laxity;
- Hyper-extensible joints (acrobatic rickets).
• Other manifestations, e.g. excessive sweating over forehead, recurrent respiratory infections, etc.
Rickets in severely malnourished children may present without clinical signs despite extensive radiological changes (atrophic rickets).
Diagnosis of rickets depends on:
• Typical clinical defomities, discussed above,
• Characteristic radio logical changes, best demonstrated at wrist joint (Fig. 6.11), showing:
- Widening of epiphyseal ends with increased space between diaphysis and epiphysis, due to poor visibility of thickened but uncalcified metaphysis.
- Fraying at the visible end of long bones, (raveled sleeve appearance), due to irregular mineralization of metaphysis.
- Cupping, i.e. concavity at the visible end of long bones, due to poor mineralization of relatively less vascular center and pressure changes.
- Splaying of the ends of long bones, due to pressure changes on poorly mineralized bones.
Other late changes include delayed bone age, costochondral widening with spatulate ribs, tri-radiate pelvis and spinal deformities.
After vitamin D administration, radiological recovery is visible in 7-10 days with appearance of provisional zone of preparatory calcification—a transverse
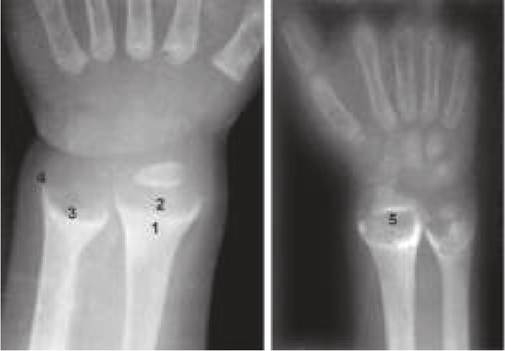
Fig. 6.11: Rickets: X-ray.
X-ray wrist showing: 1. Widening, 2. Cupping, 3. Fraying, 4. Splaying, 5. Line of preparatory calcification.
line beyond the visible end of shaft, suggestive of healing rickets. Absence of this zone after 3 weeks indicates possibility of refractory rickets.
Complete X-ray clearance takes 2-3 months, though deformities may persist for many years.• Biochemical changes depend on severity of disease and differentiate active disease from old deformities. Important changes in order of appearance are:
± Elevated S. alkaline phosphatase (gt;20 KA units) ± Low S. phosphorus levels (lt;4 mg/dl)
± Low Ca ? P index (lt;30)
± Low S. calcium levels (lt;9-11 mg/dl)
• Serum vitamin D levels [25(OH)D3] of lt; 12 ng/ml are interpreted as deficient while levels gt; 20 ng/ml are considered as sufficient (IAP guidelines 2021) in children to provide a buffer for periods of stress, exigency, and seasonal patterns.
D/D: Nutritional rickets need to be differentiated from vitamin D resistant/refractory rickets, discussed later. Some important indicators of non-nutritional rickets are given in Table 6.19.
Treatment: Conventional Stoss regimen was once the most widely used method to treat nutritional rickets and to differentiate them from resistant rickets. It involved administration of a single mega dose of vitamin D3 orally or parenterally (3,00,000-6,00,000 IU) on diagnosis along with oral calcium supplements and repeating the
TABLE 6.19: Indicators of non-nutritional rickets
• Strong family history
• Rickets within first 6 months of life
• Failure to thrive, gross muscle wasting
• Signs of renal or hepatic disease
• History of mental retardation or anticonvulsant therapy
• No response to vitamin D therapy (Stoss regimen)
• Urine: low pH, aminoaciduria, phosphaturia X-ray wrist after 2-3 weeks to see for line of preparatory calcification (Fig. 6.11). While appearance of this line indicates vitamin D deficiency rickets, absence of the line of preparatory calcification even after 3 weeks strongly indicates possibility of vitamin D resistant rickets and need for detailed investigations. However considering the potential risk of vitamin toxicity, stoss regimen is rarely used at present.
IAP guidelines 2021 recommend treatment of vitamin D deficiency with daily oral therapy with 2000 IU of vitamin D3 in infants (or 3000 IU gt; 12 months age) for minimum 12 weeks along with daily calcium intake of 50-75 mg/kg/day (max 500 mg), followed by 400-600 IU/day as maintenance dose.
However in children with poor compliance for daily therapy, infant may be given equivalent of 2000 IU/day doses on weekly/monthly basis, while children gt;12 months may be given 60,000 IU every two weeks for total 5 doses (not to exceed cumulative dose of 3,00,000 IU).
Prevention of rickets as per IAP Guidelines 2021 includes:
• Daily oral vitamin D supplementation (400 IU) in all infants lt; 1 year of age.
• No routine vitamin D supplementation is recommended beyond infancy, though adequate dietary calcium intake (500-600 mg/day; 800 mg in adolescents) and sufficient sun-exposure must be ensured. Daily sunlight exposure of 17-30 min in infants and 30-45 min in older children over 15-40% body surface area is recommended at least five times a week during noon (11AM-3PM) for preventing vitamin D deficiency across different regions and seasons.
• Routine vitamin D supplementation (400 IU/day) in children with high-risk conditions, e.g. chronic liver/renal disease, malabsorption states, chronic neuromuscular disorders and long-term therapy with anticonvulsants or steroids.
• While studies have shown lower vitamin D levels in pneumonia, tuberculosis, HIV, asthma, and ADHD/ autism, causative association is not consistent and no vitamin D supplements are recommended in these cases.
• Universal maternal vitamin D supplementation is not recommended.
6.5.2
More on the topic VITAMIN D DEFICIENCY RICKETS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- FREE RADICALS IN HEALTH AND DISEASE