Bovine Tuberculosis in Animals in Cameroon
Cameroon’s human population of over 20 million live in five agroecological zones (AEZ), namely: the (1) Sudano-Sahel (in the North and Far North regions), (2) Guinea High Savannah (in the Adamawa Region), (3) Western Highlands (in the Northwest and West regions), (4) mono-modal humid forests (in the Southwest and Littoral regions), and (5) bimodal humid forests (in the Center, East and South regions).
Over 70% of the population lives in rural areas, and their livelihood depends on crop farming and livestock rearing (Tanya 2004).The national livestock population comprises 6 million cattle (mainly indigenous, multipurpose zebu breeds), 4 million sheep, 4.6 million goats, 0.2 million horses, and about 1.8 million pigs (FAOSTAT 2014). There is also a wide range of wildlife, including predators, wild hogs, wild ruminants, and rodents inhabiting the different AEZs. The majority of livestock in Cameroon are traditionally and extensively managed, and the farmers are dependent on limited ranges and feed that are more limited during the dryer seasons and the AEZ in which they live. There is extensive transhumant movement of livestock during the dry season to cope with the feed shortage. The dominant pastoral production and extensive husbandry systems increase their vulnerability to many diseases.
Contact of livestock with wildlife (during seasonal migration) and their congregation during grazing in the field, veterinary interventions, and in livestock markets provide ample opportunity for the transmission of infectious diseases. These diseases have a huge impact on animal productivity and wellbeing; they also threaten public health because of their zoonotic transmission to humans (including BTB), with the poor being particularly vulnerable. Therefore, improved surveillance for BTB and accurate estimations of its magnitude and distribution in cattle are essential to devise appropriate intervention strategies in Cameroon.
Information on the occurrence of BTB in Cameroon is scant especially before the year 2000. Available data extracted from FAO-OIE-WHO Animal Health Yearbooks (1992-1997) and the OIE (1997-2001) confirm that BTB is prevalent in the four sub-Saharan geopolitical regions. However, a definitive regional prevalence could not be estimated due to inadequate data from several key countries such as Cameroon in the Central African region. The disease status in Cameroon is often only documented as “low and sporadic,” “disease reported,” “disease suspected but not confirmed,” and “serological evidence with no clinical disease.” No disease information was available for animals other than cattle in those reports.
Although BTB in cattle occurs widely in Cameroon, there is no structured surveillance for its presence and distribution, and information about its occurrence is mainly dependent on the detection of macroscopic lesions during the postmortal examination of carcasses and meat inspection in abattoirs (Awah-Ndukum et al. 2012b; Egbe et al. 2016). Following the provisional diagnosis of BTB during these events and immunologic reactions to ancillary tests, direct smear microscopy of Ziehl-Neelsen-stained smears of the exudate of suspect lesions, culture (on solid/ liquid media), and the results of molecular diagnostic techniques are used to confirm the presence and identification of the Mycobacterium spp. isolated from the lesions (Awah-Ndukum et al. 2013; Koro-Koro et al. 2013; Egbe et al. 2016). Intradermal tuberculin tests, immunochromatographic (lateral-flow-based rapid test), and IFN-γ assays (Bronsvoort et al. unpublished) (Awah-Ndukum et al. 2012a, b) are only occasionally used to diagnose the disease in cattle in Cameroon. In contrast to several reports from other African countries that documented BTB in other domestic animals such as pigs, small ruminants, horses, dogs, and wildlife (Cadmus et al. 2009; Hiko and Agga 2011; Hlokwe et al. 2011; Katale et al. 2012), BTB has not been detected in these animals in Cameroon.
Estimates of the national prevalence of BTB in cattle are based on opportunistic samples obtained from accessible segments of the cattle population. The distribution of the disease appears to be very patchy, and, depending on the sampling and detection methods, the prevalence varies widely from 50% (Table 12.1). Establishing the true extent of the disease will require representative samples of the total population from across the country. More often too, different prevalence estimates are reported from the same study population because of differing interpretations of the tests used, and there is a need to standardize the application and interpretation of diagnostic tests used in the country (Awah-Ndukum et al. 2012a).
| Locations | Number of animals | Prevalence (%) according to diagnostic techniques used | Reference (test interpretation standard used) |
| North and Far North regions | 890 | 10.6a; 2.7b | Martrenchar et al. (1993) (Ministry of Agriculture; France; Order: 07/11/90) |
| Northwest region | 2492 | 3a (extensive farms); 13a (Ranches) | Merlin and Tsangueu (1985) (OIE standard cut-off point) |
| West Region (experimental farm) | 142 | 14.8a (42% Zebu; 9.02% crosses) | Nfi and Ndi (1997) (OIE standard cut-off point) |
| Adamawa Region (experimental farm) | 1395 | 1.4a (Zebu cattle); 2.8a (Holstein and their crosses) | Tanya et al. (1985) (OIE standard cut-off point) |
| Northwest Region | 166 (48% exotic, 28% zebu, 20% crosses) | 26a | Muchaal (2002) (Canadian Food Inspection Agency field protocol) |
| Douala abattoir | 385,784 [1995 2003] | 0.82c | Awah-Ndukum et al. (2010) (PM detection of TB lesions) |
| Bamenda abattoir | 45,737 [1995 2003] | 0.18c | |
| Bamenda abattoir | 33,835 [2006 2008] | 0.6c | |
| Dschang abattoir | 1460 [2006 2008] | 4.2c | |
| Bamenda abattoir | 39 (zebu) | 31d | Awah-Ndukum et al. (2010) (OIE and WHO standards) |
| 51d,e | |||
| Bamenda abattoir | 90 (zebu) | 60f | Awah-Ndukum et al. (2010) (Manufacture protocol) |
| Bamenda abattoir | 163 (zebu) | 42.33c; >38d,e | Egbe et al. (2016) (OIE and WHO standards) |
| Bamenda abattoir | 1129 | 3.99c; 2.75d,e | Egbe et al. (2016) (PM detection of TB lesions; OIE and WHO standards) |
| Maroua abattoir | 175 (zebu) | 27.42c; 68.57f; 16.0d | Awah-Ndukum et al. (unpublished) |
| 85 (zebu) | 33.0c; 25.88a; 21.18b; 70.59f; 22.35d | (OIE standard cut-off point) | |
| Maroua abattoir | 122 | 14.75c; 13.1d,e | Egbe et al. (2016) (PM detection of TB lesions; OIE and WHO standards) |
| Garoua abattoir | 160 | 23.75c; 21.3e,d | Egbe et al. (2016) (PM detection of TB lesions; OIE and WHO standards) |
| Ngaoundere abattoir | 935 | 11.33c; 7.70e,d | Egbe et al. (2016) (PM detection of TB lesions; OIE and WHO standards) |
(continued)
Table 12.1 (continued)
| Locations | Number of animals | Prevalence (%) according to diagnostic techniques used | Reference (test interpretation standard used) |
| Yaounde abattoir | 319,475 [2006 2012] | rowspan=2 bgcolor=white>0.16c Awah-Ndukum et al. (unpublished) | |
| (PM detection of TB lesions) | |||
| Yaounde and Douala | 16,316 | 1.03c; 0.60d; 0.49d,e | Koro-Koro et al. (2013) |
| Yaounde abattoir | 9127 | 0.81c | (PM detection of TB lesions; OIE and WHO standards) |
| Douala abattoir | 7189 | 1.30c | |
| WHC and ADP | 2853 [2009] | 12.21a; 4.67b | Awah-Ndukum et al. 2012b (OIE standard cut-off point) |
| WHC | 2126 | 14.03a; 5.38b | |
| Adamawa (Vina) | 727 | 6.89a; 2.57b | |
| Bamenda abattoir | 129,165 [1994 2010] | 0.46c | |
| WHC and ADP | 2853 [2009] | 10.33a; 7.48b | Awah-Ndukum et al. (2012a) |
| WHC | 2126 | 5.86a; 8.63b | |
| Adamawa (Vina) | 727 | 11.86a; 4.10b | (OIE standard cut-off point and Manufacturer’s protocol) |
| WHC and ADP | 2853 [2009] | 20.18a; 5.97b | Awah-Ndukum et al. (unpublished) |
| WHC | 2126 | 11.18a; 6.97b | (OIE standard cut-off point and Manufacturer’s protocol) |
| Adamawa (Vina) | 727 | 23.25a; 3.05b | |
| WHC and ADP | 1381 [2010] | 18.35a; 7.41b | Awah-Ndukum et al. (2012a) |
| WHC and ADP | 807 | 13.14a; 3.59b; 37.17f | |
| 23.42a; 6.31b; 43.24f | (OIE standard cut-off point and Manufacturer’s protocol) | ||
| WHC | 444 (zebu/exotic) | 0.59a; 0.43b; 29.75f | |
| Adamawa (Vina) | 363 (zebu) | 24.68a; 9.89b | |
| WHC | 1018 (zebu/ exotic) |
aSIT: single intradermal tuberculin skin test
bCCT: single intradermal comparative cervical tuberculin skin test cSlaughter/meat inspection
dAFS: acid-fast staining
eLiquid/solid culture of lesions fAnti-bovine tuberculosis antibody assay (AntiBTBAb)
Year given in square bracket refers to duration of prevalence study
WHC and ADP, highlands of Cameroon (Western Highlands and Adamawa Plateau); PM postmortem
Bovine TB has been detected throughout the course of the year and the monthly prevalence ranges from 0.3 to 0.8% (Fig. 12.1). The observed increase in BTB in recent years seems to be associated with an increase in the number of cattle
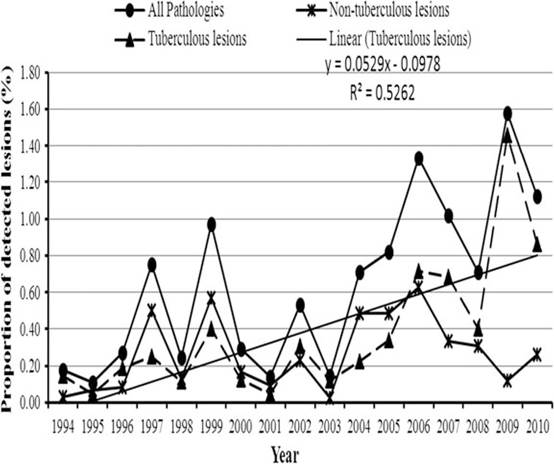
Fig. 12.1 Annual prevalence of tuberculous and non-tuberculous lesions recorded in slaughtered cattle at the Bamenda municipal abattoir, Cameroon
slaughtered and an increased efficiency of meat inspection (Awah-Ndukum et al. 2012b; Egbe et al. 2016). This increasing trend does not necessarily reflect an actual increase of the disease, but rather an improved diagnostic capability and better meat inspection procedures.
Molecular epidemiological data of BTB in Cameroon reveal a marked heterogeneity of strains with over 46 spoligotypes circulating in the country (Fig. 12.2). Mycobacteriological culture and spoligotyping confirm that though M. bovis is the principal etiological agent of BTB in Cameroon (Egbe et al. 2016; Awah-Ndukum et al. 2013), there is often a mixed and widely diverse infection of M. bovis and other Mycobacterium spp., including M. tuberculosis, M. gordonae, M. phlei, M. fortuitum, M. mucogenicum, and M. scrofulaecum (Egbe et al. 2016). The extent of their contribution to the disease burden is unknown, and confirmation of the cause of tuberculous lesions by mycobacteriological and molecular diagnostic techniques is essential to establish their importance.
For effective surveillance of BTB in Cameroon, meat inspection should be supported by tracing-back suspicious cases to the herds of origin to allow appropriate measures such as isolation and slaughter, and restriction of movement to other herds, to be instituted to limit further spread of the infection.
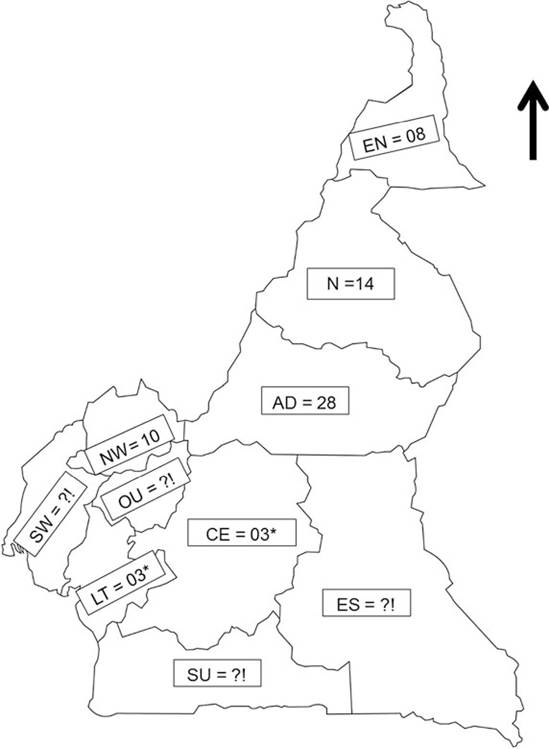
Fig. 12.2 Geographical distribution of the 46 M. bovis spoligotypes isolated in Cameroon. (1) Regions of Cameroon: EN (Far North); N (North); AD (Adamawa); NW (North West); OU (West); SW (South West); LT (Littoral); CE (Centre); SU (South); ES (East); (2) AD = SB0300, SB0893, SB0954, SB0955, SB1027, SB1099, SB1104, SB1418, SB1462, SB2313, SB2316,
SB2317, SB2318, SB2319, SB2320, SB2321, SB2323, SB2327, SB2328, SB2330, SB2331,
SB0944, SB0951, SB0953, SB1025, SB1460, SB2033, SB2162, SB2324; (3) EN = SB0944, SB0951, SB1460, SB1459, SB2325, SB2332, SB2333, SB0952; (4) N = SB0944, SB0951,
SB1025, SB1460, SB2033, SB2324, SB1459, SB0120, SB2329, SB2334, SB2035, SB0952,
SB1461, SB1463; (5) NW = SB0944, SB0953, SB2162, SB1026, SB2035, SB2161, SB2163, SB2164, SB2314, SB2315); (6) CE and LT = SB2033, SB2035, SB1419; (7) ?!: No data available (SW, OU, SU and ES are not major cattle producing areas); (8) *: cattle slaughtered in LT and CE mainly originate from AD, N, NW; (9) Spoligotype patterns were named according to www. Mbovis.org International database (Smith and Upton 2012). (Sources: Egbe et al. 2017; Awah- Ndukum et al. 2013; Koro-Koro et al. 2013; Njanpop-Lafourcade et al. 2001)
12.3