canine Parvoviral enteritis
NICOLA DECARO AND CANIO BUONAVOGLIA
Department of Veterinary Public Health, Faculty of Veterinary Medicine of Bari, Valenzano (Bari), Italy
AETIOLOGY
Canine parvovirus 2 (CPV2) is an autonomous parvovirus that is genetically and antigenically unrelated to the first described parvovirus of the dog, Canine parvovirus 1 (CPV1), or minute virus of canines.
CPV2 belongs to the feline parvovirus group within the genus Parvovirus, together with Feline panleukopenia virus (FPLV) and other parvoviruses of carnivores. The original type CPV2, firstly identified in the late 1970s, was completely replaced a few years after its emergence by two antigenic variants, CPV2a and CPV2b, and no longer circulates in the field. CPV2a and CPV2b are variously distributed in the canine population worldwide. More recently, a third antigenic variant, CPV2c, has been reported, firstly in Italy, and has subsequently been shown to be distributed worldwide.epidemiology
The three antigenic variants have a variable distribution in domestic dogs in different areas of Europe, with an approximately equal detection of CPV2a and CPV2c in Italy, Germany, Spain and France, and detection of CPV2a in Belgium and eastern Europe and of CPV2b in the UK(1), (Figure 12.1).
CPV2 infects primarily domestic dogs (Canis famil- iaris), and the target canine population is represented mainly by pups aged between 4 and 12 weeks, when the maternally derived antibodies (MDA) wane. However, recently multiple outbreaks of CPV2 disease have been reported in adult dogs, and even in dogs regularly vaccinated. In contrast to the original CPV2, the antigenic variants can infect and cause disease in domestic and wild cats. CPV2 has been reported in European wild species of the Canidae family, especially wolves ( Canis lupus) and red foxes (Vulpes vulpes). Clinical outbreaks of CPV2 infections in wolves (Canis lupus) have been reported in the USA, and parvovirus infection has been associated with a decline in the wolf population in Minnesota.
In European free-ranging wolves, the virus has been detected only spo-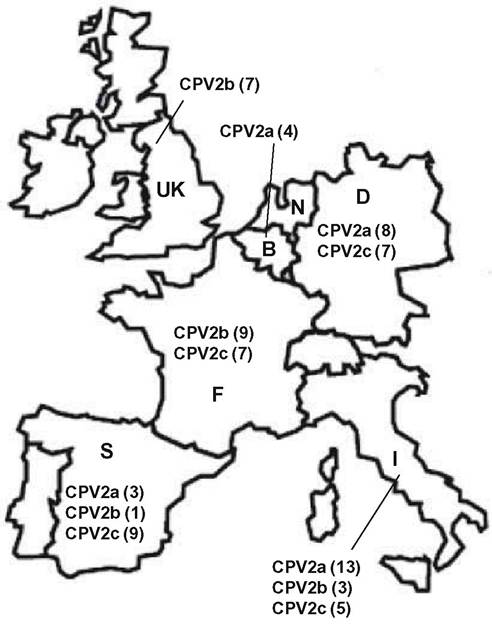
FIGURE 12.1 Geographic distribution of the antigenic variants of Canine parvovirus 2 (CPV2) in domestic dogs in Europe (adapted from Decaro et al, 2011(1)). The CPV variants are indicated for each country by numbers in parentheses.
radically(2) while the same CPV2b strains were found to circulate in both domestic and wild canids(3). However, the circulation of CPV2 in European wolves has been proven by serological investigations. The CPV2 seroprevalence in these canids was 62.2% in Spain(4) and 32.% in Portugal1-5). Red foxes were found to be infected by viruses intermediate between CPV2 and FPLV, which accounts for their closer phylogenetic relatedness to felids with respect to other Canidae. Accordingly, parvoviruses isolated from blue foxes (farmed Alopex lagopus) and named Blue fox parvovirus (BFPV) were characterized as true FPLV(6). European red foxes displayed lower CPV2 seroprevalence rates than wolves, with values of 5—12% in Spain(4’7), of 9.1% in Portugal1-5), and of 9—13% in Germany(8). CPV2a sequences were identified in a stone marten (Martes foinaff whereas an outbreak of CPV2 infection occurred in farmed raccoon dogs (Nyctereutes procyonides) in Finland(9). Exposure to CPV2 or to related viruses has been also demonstrated in free- ranging Marsican brown bears (Ursus arctos marsicanus) in Italy1-10), raccoon dogs and pine martens (Martes martes) in Germany)8), Egyptian mongooses (Herpestes ichneumon) and common genets ( Genetta genetta) in Spain(7).
CPV2 is highly contagious and can be transmitted through direct contact with infected animals or — most frequently — by indirect contact, with their faeces.
The faeces of the infected animals are highly infectious and may contain billions of CPV2 virions per gram, thus representing the main source of environmental contamination. The faecal shedding may persist for several weeks and, due to its exceptional stability, the virus can remain infective for some months in the environment.PATHOGENESIS, PATHOLOGY AND IMMUNITY
The pathogenesis of the CPV2 infection in wildlife is poorly known, but it has been extensively investigated in domestic dogs. The target tissues are the intestinal crypts and the lymphoid organs. The virus penetrates through the oronasal route and replicates primarily in the lymphoid tissues of the oropharynx, mesenteric lymph nodes and thymus. After this first-round replication, CPV2 causes leucocyte-associated viraemia and the virus disseminates to the germinal epithelium of the crypts of the small intestine which produces the cells that migrate to the intestinal villi and develop to mature enterocytes. The onset of diarrhoea is due to the massive lysis of these cells and subsequent impairment of the cell turnover at the tips of the intestinal villi. The virus also infects white blood cells, mainly lymphocytes, and lymphoid cells in thymus, lymph nodes and bone marrow. The virus-induced acute lymphopenia (often associated with neutropenia) is responsible for the impairment of the immune response against common pathogens. This impairment may lead to secondary infections, which in turn exacerbate the clinical course of the disease. In 2- to 3-week-old pups, CPV2 is also able to replicate in the cardiac cells, inducing a fatal myocarditis.
Post mortem findings of CPV2 infection in domestic dogs are represented by haemorrhagic enteritis of the small intestine. Mesenteric lymph nodes and Peyer’s patches are usually haemorraghic, while the thymus can be atrophic. In the cardiac forms, the heart walls can be flaccid and pale streaks are often evident in the myocardium. Sometimes, areas of patchy consolidation are visible in the lungs as a consequence of pneumonia induced by opportunistic pathogens.
Histopathology reveals the presence of multifocal crypt necrosis, intranuclear inclusion bodies in the small intestine and necrosis of lymphoid tissues with depletion of lymphocytes in Peyer’s patches, lymph nodes, spleen and thymus. Myocarditis with viral inclusion bodies may be present in young pups. Gross and microscopic lesions in wild canids are similar to those observed in domestic dogs.Antibodies appear very rapidly after infection, peak 7—10 days post- infection and persist for at least 2 years. Haemagglutination-inhibiting antibody titres ≥1r80 protect dogs against CPV2 infection and disease, whereas titres between 1:20 and 1:40 are able to protect against disease but not against infection. The cell response against CPV2 is poorly studied; however, protection of pups recovered from CPV2 infection is life-long.
CLINICAL SIGNS AND TREATMENT
In domestic dogs, haemorrhagic enteritis is the predominant clinical form observed during CPV2 infection, but the severity of the disease may vary on the basis of titres of MDA still present in the infected pups. After an incubation period of 3—7 days (which can be shorter for the antigenic variants), the infected pups display loss of appetite, depression, vomiting and diarrhoea, which can range from mucoid to bloody. Dehydration and fever can also occur. Currently myocarditis in young pups is only sporadically observed, as most pups have MDA titres that protect them in the early stage of life. Leucopenia is a constant finding of CPV2 infection, with white blood cell (WBC) counts dropping below 2000—3000 cells∕μl of blood. Both neutrophil and lymphocyte counts decrease, but lymphopenia is more pronounced. Sometimes the total WBC counts are within normal ranges, as a result of the simultaneous onset of lymphopenia and neutrophilia. The impairment of the immune response can also predispose to bacterial infections of the respiratory tract, with the occurrence of respiratory distress.
Subclinical and unapparent infections are frequently detected, mainly in pups with intermediate MDA titres and in adult dogs. The mortality rates can be high (up to 70%) in pups, but are usually less than 1% in adults dogs. Although some viral isolates from European wild carnivores have been characterized at the molecular level, there are no reports on the clinical findings of CPV2 infection in free-ranging animals and only one report exists on the disease observed in farmed raccoon dogs in Finland. In these outbreaks, 3- to 5-week-old pups were affected, displaying acute gastroenteritis with vomiting and diarrhoea of variable severity1-9). Other wild canids were found to be clinically affected in North America and the clinical signs observed were the same as in domestic dogs. A suspected (but unconfirmed) case of CPV2 acute myocarditis preceding the onset of canine distemper was reported in a 1.5-year-old Eurasian badger (Meles meles) in Austria1-11).Treatment of CPV2 infection in infected carnivores is essentially based on the administration of fluids to restore the electrolyte balance and antibiotics when secondary bacterial infections occur. Administration of hyperimmune sera is not recommended to reduce the clinical course of CPV2 infection but only to confer a short-term protection in the case of possible contacts with infected animals.
DIAGNOSIS
Canine parvoviruses are highly stable in the environment and are able to cause haemagglutination in vitro only at temperatures below 5° C, and this property is routinely employed for diagnostic purposes. CPV2 can replicate i n vitro on cell lines of canine and feline origin, such as canine mammary fibroma (A-72), Crandell feline kidney (CrFK) and Felis catus whole fetus (fcwf) cells.
Haematology can be useful for detection of the CPV2- induced lymphopenia, which may have prognostic relevance. A definitive diagnosis of CPV2 infection is mainly based on the detection of the virus, viral antigens or nucleic acid in the faeces of the animals with clinical signs.
Virus detection in faecal samples is traditionally made by using electron microscopy, virus isolation on susceptible cell lines, haemagglutination in the presence of pig or cat erythrocytes, and in-house tests based on immunochromatography. As these assays have been proven to be poorly sensitive, especially in the late stages of infection, molecular assays have been developed for detection of the CPV2 DNA in clinical samples. Apart from conventional polymerase chain reaction (PCR) protocols, a real-time PCR assay exists for detection and quantification of CPV2 DNA. More recently, type-specific minor groove binder (MGB) probe assays were developed for specific characterization of the various CPV2 variants and for discrimination between vaccine and field strains. Serological methods (haemagglutination inhibition and virus neutralization tests) are not useful for CPV2 diagnosis, but they can be successfully employed for the titration of MDA interfering with active immunization of pups and for seroepidemio- logical surveys in wildlife.MANAGEMENT, CONTROL AND REGULATIONS
Prophylaxis of CPV2 infection in domestic dogs is carried out by means of extensive vaccination. Both inactivated and modified live virus (MLV) vaccines are available. Killed formulations have been proven to induce only short- term immunity, so MLV vaccines are more widely used in domestic dogs. CPV2 vaccines are prepared by using either the original type CPV2 or its variant CPV2b. Currently, there are some concerns about the complete efficacy of type-2-based vaccines against the antigenic vari- ants(12). Vaccines should be administered only after waning of MDA in order to avoid the interference with active immunization of pups. Vaccination of free-ranging carnivores is usually not possible, but it should be performed every time there is an opportunity and is mandatory when a captive-born canid is reintroduced into its natural habitat. Vaccination is also recommended for wild canids living in peri-urban areas that may have multiple contacts with CPV2-infected domestic dogs(6).
SIGNIFICANCE AND IMPLICATIONS FOR ANIMAL HEALTH
There are not enough data to assess whether CPV2 circulates independently in wild carnivores or whether the virus circulation in these animals is limited to sporadic contacts with infected domestic dogs. A role for wildlife reservoirs in the emergence of CPV2 has been proposed, but conclusive evidence is not yet available.