Ear Mites
Ear mites are the most common parasites found in the ear canals of dogs and cats. We are all too familiar with Otodectes mites causing severe damage to the lining of the ear canal, with the resulting “coffee grounds” exudate composed of wax, blood, and epithelial cells.
The ear mite has been identified in a number of animal species, both domestic and wild. A nonburrowing psoroptic mite, the ear mite feeds on epithelial cell lymph and blood. They have chewing mouthparts that can cause damage to the epithelium. In dogs and cats, ear mites can cause a severely pruritic parasitic otitis that is commonly associated with a bacterial infection and otitis media.A unique result of Otodectes infestation in the cat is a systemic hypersensitivity reaction. Known as otodectic mange, this skin disease resembles miliary dermatitis, a papular, crusty eruption found around the neck and head, dorsolumbar area, and inguinal area. When an ear mite-infected cat sleeps with its ear in the flank, the ear mites can leave the ear canal and get on the skin. A similar transfer occurs when an infected cat scratches the ear and the mites get on the paw. Those mites in an ectopic location migrate along the skin and feed. This results in a hypersensitivity reaction to the mite antigens absorbed across the damaged epithelium. Experimentally, infected cats showed an immediate hypersensitivity reaction to an intradermal mite extract. Cats infected for 35 days showed an Arthus (Type III) reaction. Serum precipitating antibodies were noted 45 days after infection. When cats with miliary dermatitis do not respond to systemic steroids, such as methylprednisolone acetate (DepoMedrol, Pfizer), or to flea-control measures, otodectic mange should be considered and the cat should be treated for Otodectes using a systemic acaricide such as ivermectin, fipronil, or sealmectin.
A cat affected with ear mites shakes its head violently and scratches at the ears. Facial abrasions and hair loss may be evident between the lateral canthus of the eyelid and the ear. When examined, the ear canals display the typical reddish-brown to black, dried, crusty exudates. The brown color is presumed to be from dried wax mixed with blood products. On otoscopic examination, the mites can be seen as white insects crawling on the surface of the exudates.
If the otoscope is held very steady, the mite activity increases, because the light arouses the mites and makes them more active. When viewed with a video otoscope (Video Vetscope, MedRx, Inc., Largo, Florida), which has a high magnification and a bright light source, the mites can often be seen in colonies, with thousands of mites scurrying about (Figure 5-1).
In cases of ear mites in dogs, only a few mites may inhabit the ear canal. They often elude otoscopic or microscopic detection. It has been theorized that either severe inflammation in the ear drives the mites out of the ear or the exudates in the ear canal destroy them. In either case there is a local immune response to mite antigens in the dog’s ears that makes the environment hostile to the mites. The severity of the symptoms associated with Otodectes may be due to the Arthus-like immediate hypersensitivity reaction provoked by the presence of very few mites.
One useful technique for diagnosing ear mite infection in patients in which Otodectes is suspected but no mites are seen otoscopically is a mineral-oil roll smear.
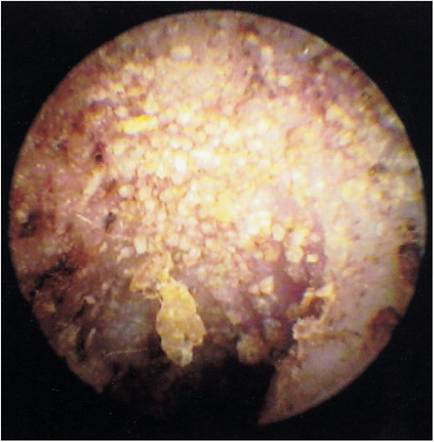
Figure 5-1
Otoscopic view of a cat's ear filled with hundreds of Otodectes mites. The dry, flaky ceruminous exudate is forming a crust in the ear canal.
A small cotton-tipped applicator is saturated with mineral oil and is used to swab out the exudates in the ear canal. The cotton tip is then placed into a drop of mineral oil on a microscope slide, and the tip is rolled back and forth to remove most of the harvested material from the cotton tip onto the slide.
The slide is then coverslipped and examined under low-power (40? to 100?) magnification. Adult mites individually, or often in duos representing breeding pairs, can easily be seen crawling through the microscopic field. When few mites are present in the ear canal, the typical long oval brown eggs of Otodectes may be the only evidence of infection (Figure 5-2).The ear mites live primarily in the ears, where they feed with their chewing mouthparts on epithelial cells and blood. Female Otodectes mites lay solitary eggs in the ear canal, and within 2 or 3 weeks of maturation adult mites begin feeding. Ear mites are very prolific, and in a short time after infection the mite infestation may be severe.
Although ear mites can live in the environment for a short time, direct transmission of Otodectes from animal to animal is accepted as the usual mode of transmission. Mites can jump onto any part of the body and then migrate into the ear canal. Many affected 6-week-old kittens have severe ear disease because they acquired Otodectes from their queens during the neonatal period. In situations of high animal density, such as shelters, pet shops, and breeding colonies, ear mites can affect the entire population. It is rare for a noninfected, solitary, indoor cat to acquire ear mites.
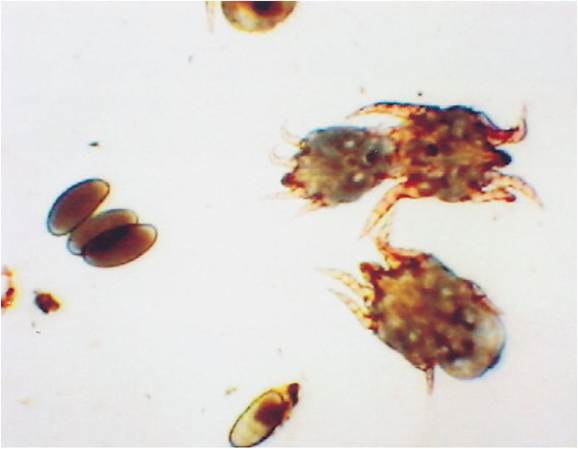
Figure 5-2
Otodectes mites in a mineral-oil swab of otic exudates. The presence of typical dark brown oval eggs of Otodectes may be the only indicator of infection in the absence of adult mites.
The aggressive feeding habits of Otodectes cause damage to the epithelium of the ear canal and the tympanic membrane. Ceruminous gland secretion is increased and contributes to the quantity of the exudates. Secondary bacterial infection may result from the loss of the protective epithelial barrier in the ear canal; a contributing factor is the high serum-protein substrates that are made available to the bacteria as a result.
Damage to the germinal epithelium on the surface of the eardrum from ear mites prevents these cells from sliding across the eardrum as a cleansing mechanism. This results in the accumulation of waxy material on the eardrum, producing a wax plug. Ear mites at the eardrum can actually chew their way through the thin tympanic membrane and invade the middle ear, resulting in otitis media. Whether ear mites that reach the middle ear can be involved in the formation of nasopharyngeal polyps has yet to be determined.Treatment of Otodectes has traditionally involved the use of ear drops containing a variety of insecticides in a number of different vehicles. Thorough cleaning of the ear canal, preferably with the patient sedated prior to the use of any topical medication, hastens the therapeutic effects of the topical medication. All ear mite medications contain insecticides, which are placed in the ear to kill the mites. Some preparations contain additional ingredients such as (1) ceruminolytics to help loosen the inspissated ceruminous material, (2) antibiotics to treat secondary bacterial infection, and (3) mineral oil, which is used as a vehicle to float the debris to the pinnal surface so it can be removed. Mineral oil may also have the beneficial effect of blocking the breathing tubes of the mites and suffocating them. Drops for ear mite infections need to be used for at least 14 days so that the mites hatching in the canal are killed before the life cycle starts over. Retreatment at monthly intervals has been recommended for free-roaming cats with chronic mite infestations.
Because the anthelmintic ivermectin has been demonstrated to be a good acaricide as well, it has been used for treatment of ear mites in dogs and cats. Ivermectin is only approved for use in dogs as a heartworm preventative. Injectable ivermectin (Ivomec 1% injection, Merial, Ltd.) is used at a dose of 250 μg∕kg or 0.1 ml/10 lb of body weight. It is injected subcutaneously every 10 days to 2 weeks for two or three injections.
Because it is well established that ear mites can live on the skin, these injections treat the entire body. All contact animals in the environment should be treated concurrently. Ivermectin can also be placed in each ear canal as a topical treatment for ear mites, but this preparation contains propylene glycol, which can be irritating to the ear canal.Some severe neurological reactions and even deaths have been reported in cats treated with injections of ivermectin. Kittens under 12 weeks old treated with injectable doses that exceed 250 μg∕kg may be more susceptible to the fatal reactions than adult cats. The reason for this may be linked to the age at which the blood-brain barrier develops in kittens. It is hypothesized that without an adequately mature blood-brain barrier, ivermectin can gain access to the brain in affected kittens and interact with gamma-aminobutyric acid (GABA) receptors in the brain, causing neurological signs to develop. Because of this, a topical aqueous ivermectin 0.01% solution (Acarexx, Idexx) has been developed for use in the ears of kittens 4 weeks of age and older. Another topical aqueous ear mite formulation safe for young kittens is a 0.1% milbemycin oxime solution (Milbemite, Novartis). These aqueous topical ear mite preparations are packaged in individual foil packs containing 0.5 ml of solution in two premeasured plastic applicator ampules.
Fipronil (Frontline TopSpot, Merial, Ltd.) and selamectin (Revolution, Pfizer) are monthly flea-control topical preparations that have demonstrated miticidal activity in both dogs and cats. In areas with high flea infestation rates, the use of either of these flea-control products may also aid in treatment of Otodectes. Free-roaming pets with these insecticides on their skin may acquire new Otodectes mites on their skin, but the mites will be killed by the residual insecticide prior to reproducing. This may act as a preventative against ear mites.
Treatment for otitis externa secondary to Otodectes infection must not be overlooked. Antibiotic and antibiotic-steroid ear drops are used until the epithelial surface heals and the infection subsides. If otitis media is present, the ear canal and the tympanic bulla should be flushed and suctioned carefully to remove any debris that may have gained access to the tympanic bulla.