Introduction
An effusion is an abnormal accumulation of fluid within a body cavity (Beatty & Barrs, 2010; Dempsey & Ewing, 2011; Gavazza et al., 2013; Valenciano et al., 2013) (Table 15.1).
In health, a small amount of fluid between the parietal and visceral surfaces of body cavities acts as a lubricant to facilitate the motion of internal organs against each other and the body cavity walls (Dempsey Ewing, 2011). Within the pleural space, fluid-mediated adhesion of lungs to the chest wall allows mechanical coupling for a direct transmission of forces for normal respiration (Dempsey Ewing, 2011). Visceral and parietal surfaces are lined with mesothelial cells. Mesothelial cells are arranged in a pavement-like monolayer on a basal membrane. They play a pivotal role in fluid and cell transport across the serosal cavities, antigen presentation, inflammation, tissue repair, coagulation and fibrinolysis, and tumor cell adhesion. Mesothelial cells are derived from the mesoderm but exhibit mesenchymal and epithelial characteristics by expressing desmin, cytokeratin, and vimentin intermediate filaments (Mutsaers, 2004; Reggeti et al., 2005). They typically develop epithelial or fibroblast morphology and phagocytic activity with specific inflammatory stimulation (Reggeti et al., 2005). In health only 0.16–0.5% of cells undergo mitosis at any one time, but in cases of injury, the mitotic rate increases dramatically by up to 30–80% on the wound edge. Mesothelial healing is different from other true epithelial surfaces as it occurs diffusely across the wound and not continually from the wound margins toward the center (Mutsaers, 2004). The mesothelium provides a protective barrier against physical damage and invading organisms. Mesothelial cells are connected by tight junctions and secrete glycosaminoglycans, predominantly hyaluronan, which forms a protective coat against microorganisms and tumor cells (Mutsaers, 2004; Dempsey & Ewing, 2011). They also have fibrinolytic activities to prevent the formation of fibrous adhesions (Mutsaers, 2004; Dempsey & Ewing, 2011).Table 15.1 Classification of effusions
| Effusion | Appearance | TP | TNCC | Cytology | Other tests |
| Normal fluid | Light yellow, clear | 3.5 g/dl | >5 ? 103/μl | Low glucose concentration | |
| Septic exudate | Beige, brown to green, flocculent, smelly | >3.5 g/dl | >5 ? 103/μl | Degenerate neutrophils; infectious agents visible | Low glucose concentration |
| FIP-associated exudate | Yellow, clear, high viscosity, tends to clot | >3.5 g/dl, usually much higher | Low | Protein precipitates with cracked glass-like appearance; cells do not spread so identification is difficult | High globulin concentration; low albumin:globulin ratio |
| Hemorrhage (acute) | Shades of red | Usually >3.5 g/dl | Comparable to peripheral blood | Platelets absent | |
| Hemorrhage (chronic) | Shades of red | Variable, depending on dilution | Variable | Platelets absent | |
| Chylous (early) | Milky, white opaque | >3.5 g/dl | >5 ? 103/μl | Small well-differentiated lymphocytes; cytoplasmic lipid vacuoles in all types of cells but predominantly in macrophages presence of chylomicrons | Triglyceride concentration > 100 mg/dl |
| Chylous (late) | Milky, white opaque | >3.5 g/dl | >5 ? 103/μl | Increasing number of neutrophils and macrophages exceeding the small well-differentiated lymphocytes; cytoplasmic lipid vacuoles in all types of cells but predominantly in macrophages Presence of chylomicrons | Triglyceride concentration > 100 mg/dl |
| Lymph | Clear slightly turbid | Variable higher than transudate | Variable but increased | Predominantly small lymphocytes | Absence of chylomicrons |
| Pseudochylous | Stable turbidity, slightly yellow | Variable but higher than transudates | Variable but mostly increased | Pyknotic cells | Cholesterol concentration > plasma cholesterol |
| Bilious effusion | Green to yellow orange, mucinous strands | Variable but higher than transudates | Variable but mostly increased | Bilious mucus and biliary pigment; variable inflammatory cells | Bilirubin concentration > plasma bilirubin |
| Uroperitoneum (early) | Yellow, clear | Low | Low | ||
| Uroperitoneum (late) | Yellow, clear | Low | Low | Unremarkable | Creatinine >> plasma creatinine |
| Viscous rupture | Turbid, flocculent, odorous | Mixed bacterial population may be present; feed material may be detected | |||
| Neoplastic | Variable | Variable | Variable | Tumor cells present | None |
| TP, total protein; TNCC, total nucleated cell count. | |||||
Normal body cavity fluid is a clear, colorless to yellowish, low protein plasma dialysate with a low cellularity.
Its formation is regulated by a delicate balance between hydrostatic and oncotic forces within the capillary bed, interstitial fluid, mesothelial and endothelial permeability, and integrity of lymphatic drainage. The lymphatic vessels communicate directly with body cavities through openings, called stomata (mouths), which are the only openings wide enough to allow cells and larger molecules to exit the vessels.The chemical composition of body cavity fluids is determined by the permeability of capillary walls, which can be passed by nonprotein solutes such as glucose, urea, creatinine, electrolytes, bicarbonate, calcium, and phosphate. The small amount of protein in normal body fluids is derived from interstitial fluid. Protein concentration in interstitial fluid varies between tissues. It is lowest in skeletal muscle (1.5 g/dl [15 g/l]) and highest within the liver (6 g/dl [60 g/l]). Normal body cavity fluid has a protein concentration Rebar, 2016).
The conventional approach to differentiate transudates from exudates by fluid total protein concentration and nucleated cell count and/or neutrophil concentration (percentage) has been challenged by recent research because evidence-based data for the conventional approach are lacking (Zoia, Petini et al., 2020). The respective cut-offs for TP and TNCC differ markedly among references and contradictory results such as a high TNCC combined with a low protein concentration are common. Particles such as cell aggregates or coagulated material either present within the effusion or forming when diluted with hematology analyzer reagents might interfere with automated cell counts. (Giordano et al., 2015) Therefore some authors consider chemical assays to be more sensitive in identifying exudates, but as such less specific, than conventional classification schemes. ‘Light’s criteria’, a dichotomous classification system based solely on biochemical tests, has been adopted from human medicine and applied to canine and feline pleural effusions (Zoia & Drigo, 2016; Zoia, Petini et al., 2020).
In human medicine Light’s criteria are used to differentiate between transudative or exudative pleural fluid which is of imminent importance in detecting tuberculosis-associated pleural effusions. Light’s criteria combine measurements of lactate dehydrogenase activity (LDH) and total protein (TP) concentration in simultaneously collected samples of the effusion and patient’s serum/plasma. A ratio (LDHr) is calculated by dividing LDHeffusion by the LDH activity of serum. An LDHr > 0.6 indicates an exudative effusion. The rationale behind LDH activity measurement is the ubiquitous activity of LDH within all cells; it is as such a surrogate marker for cellularity. Serum should be preferred because high LDH activity within platelets might falsely increase LDH activity in plasma samples. Other preanalytical conditions such as even minor blood contamination of body cavity fluid by sampling or micro- (invisible) hemolysis of serum samples might yield erroneous results in LDH measurements. A TPr (TP concentration of the effusion divided by serum protein concentration) is calculated accordingly to differentiate a protein-rich transudate caused by increased hydrostatic pressure from a pure transudate caused by decreased oncotic pressure. In protein-rich transudates the TPr exceeds 0.5. Light’s criteria have been applied in their original as well as modified versions or combined with other tests. Acquisition of simultaneous serum samples might restrict their clinical usefulness. Performance of single or combined biochemical measurands such as lactate dehydrogenase activity (LDH) (Smuts et al., 2016), cholesterol and albumin concentrations (Alonso, Mattoso et al., 2021), or lipoprotein profiles (Alonso, Behling‐Kelly et al., 2022) have also been investigated to aid differentiation between exudates, pure transudates, and protein-rich transudates. However, lipoprotein profiles did not add much value to the total protein measurement (Alonso, Behling‐Kelly et al., 2022). A correct diagnosis can only be established when clinical data, patient history/medication, and laboratory test results are reasonably combined and should not be based solely on isolated laboratory test results. A case-oriented holistic approach where all these previously mentioned factors are considered will yield more accurate results than strictly following the conventional classification scheme of transudates, protein-rich transudates, and exudates (Athanasiou, 2019).Transudates
Transudates form because of an increased hydrostatic pressure with or without a decreased oncotic pressure (hypoproteinemia/hypalbuminemia) and/or blocked lymphatic drainage (Stockham & Scott, 2013). Increased hydrostatic pressure can occur because of congestive and, especially, right-sided heart failure or mechanical obstruction of the venous outflow. The amount of protein spilling into the body cavity depends on the protein content of the interstitial fluid of the organ, which is mainly affected by the increase of hydrostatic pressure (see above). An increase in post-sinusoidal hydrostatic pressure leads to the formation of a protein-rich transudate, because the protein concentration in hepatic interstitial fluid almost meets serum plasma protein concentration. Protein-rich transudates are most commonly caused by congestive heart failure (mostly right-sided heart failure in dogs). In cases of severe hypoproteinemia (e.g. hepatic fibrosis or protein-losing pathologies), even a post-sinusoidal transudate will have a low protein concentration, which complicates its identification as such (Stockham & Scott, 2013).
Disorders resulting in portal hypertension represent another mechanism for transudate formation. These diseases can be classified by overlapping systems. The vascular system identifies the lesions as pre-sinusoidal, sinusoidal, and post-sinusoidal, and the anatomic system classifies them as luminal (e.g. thrombosis) or extraluminal (Stockham & Scott, 2013).
In dogs, the most common causes for the formation of protein-poor transudates are hepatic fibrosis and protein-losing diseases (more commonly nephropathies than enteropathies). Another mechanism for transudate formation is a decrease or cessation of lymphatic drainage. This might occur with protein-losing enteropathies or diseases of internal lymph nodes.The body cavity fluid from healthy animals is a clear, light yellow, low protein plasma dialysate, which contains only a few nucleated cells consisting of mononuclear cells such as macrophages, small lymphocytes, and mesothelial cells, and a few nondegenerate neutrophils. Transudates are of similar composition, but cellularity is probably at least in the beginning lower due to dilution. When serum protein concentration is within the reference interval for the species, the increase of hydrostatic pressure will incite transudation, whereas the protein content of the transudate will be influenced by the protein concentration of the interstitial fluid of the organ in which the hydrostatic pressure is increased (see above).
Exudates
Exudates form as a sequela of increased vascular and mesothelial permeability caused by inflammation. This type of effusion is rich in proteins and cells, predominantly neutrophils, which permeate the capillary walls and invade the respective body cavity.
Septic exudates
Septic exudates are caused by bacterial, viral, fungal, or protozoal infections. The detection of infectious agents by microscopic evaluation can be difficult; therefore cytologic features such as the presence of degenerate neutrophils should be complemented by bacterial culture. Depending on the type of bacteria involved and their toxin production, degenerate neutrophils will occur (Figures 15.1–15.5). Some bacteria species such as Nocardia or Actinomyces cause only mild degeneration of neutrophils in close proximity (Thompson & Rebar, 2016). Phagocytized bacteria will be most readily detected in the marginal areas of a cytospin preparation or feathered edge of a smear. In septic effusions the background might change from clear to smudged, with an increase of precipitates and cellular debris. Bacterial peritonitis can be categorized into primary and secondary forms (Culp et al., 2009). Primary bacterial peritonitis is defined by infection of the peritoneal cavity without an identifiable intraperitoneal source of infection, whereas in secondary bacterial peritonitis a penetrating injury can be confirmed (Culp et al., 2009). Bacterial translocation penetrating a functionally defective intestinal wall is theorized as an inciting mechanism for primary septic peritonitis. In dogs and cats with primary bacterial peritonitis, mostly Gram-positive bacteria and often only a single species were cultured in the majority of cases, whereas Gram-negative and multi-species culture predominated in secondary bacterial peritonitis (Culp et al., 2009). Bartonella spp. are bacteria that do not conform to the paradigm of septic exudates, as they produce protein-rich transudates by damaging endothelial cells and thus increasing capillary permeability (Cherry et al., 2009). These organisms require advanced culture technique or molecular methods for detection and should be considered as a differential, when no other cause for an effusion can be identified.
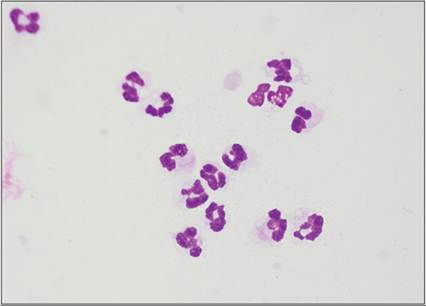
Figure 15.1 Septic exudate from a dog, containing high numbers of degenerate neutrophils. The chromatin is smudged with nuclear swelling with cytoplasmic vacuolization (Hemafix™, 1,000? magnification).
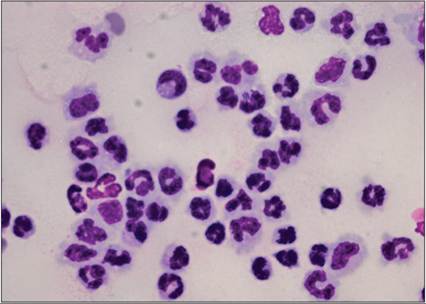
Figure 15.2 Septic exudate from a dog. Degenerate neutrophils and many intra- and extracellular rod-shaped bacteria are observed (Hemafix™, 1,000? magnification).
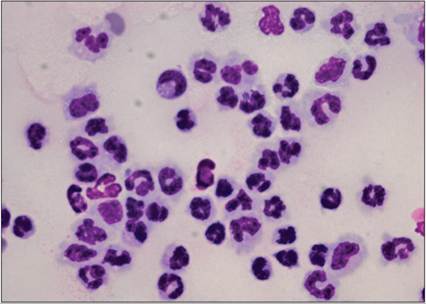
Figure 15.3 Septic exudate from a dog. Rare intracellular rod-shaped bacteria are present (center, top, right) (Hemafix™, 1,000? magnification).
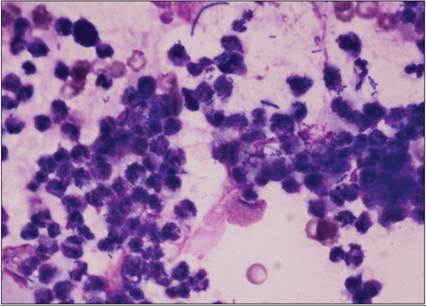
Figure 15.4 Abdominal effusion from a dog. Many degenerate neutrophils are observed with a mixed population of rod and cocci bacteria. Because of the mixed population of bacteria, there is concern for gastrointestinal perforation or leakage (Hemafix™, 1,000? magnification).
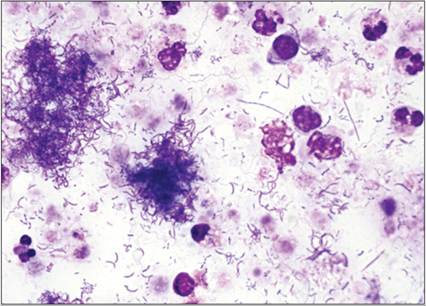
Figure 15.5 Direct smear from an abdominal effusion from a dog. Note the mixed bacterial population within the background. Rods, cocci, and filamentous rods are observed (Hemafix™, 1,000? magnification).
Nonseptic exudates
Nonseptic exudates can form because of necrosis due to ischemia, anatomic dislocations, irritating sterile body fluids due to rupture of viscera (bile, urine), sterile foreign bodies (surgical sponges), or neoplasia.
Feline infectious peritonitis
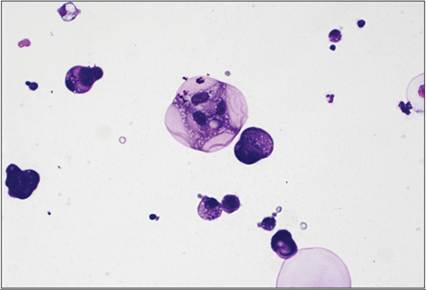
Feline infectious peritonitis (FIP)-associated effusions are high-protein exudates with low cellularity (Figures 15.6, 15.7). They are caused by a viral-induced vasculitis, which allows large proteins to enter the body cavity fluid, whereas the cells remain within the tissue forming the characteristic perivascular granulomas. Vascular endothelial growth factor produced by FIP virus-infected macrophages/monocytes increases vascular permeability and correlates with the amount of fluid produced in the course of the disease (Takano et al., 2011). A pinkish background with cracks resembling broken glass and cells that are not spread out well, so that it is difficult to recognize the segmented nuclei of neutrophils, is a typical finding in FIP-associated effusions (Figures 15.8, 15.9). The Rivalta test, a simple protein precipitation test, has been proven useful in indicating suspect FIP in effusions (Fischer, Sauter-Louis et al., 2012; Fischer, Weber et al., 2013; Barker & Tasker, 2020). In a large study of 851 feline patients from which 782 had conclusive test results, a diagnostic sensitivity of 0.91 and a specificity of 0.66 were reported (Fischer, Sauter-Louis et al., 2012). Briefly 20 µL of 100% acetic acid are added to 7 mL of distilled water and thoroughly mixed. 20 µL of the effusion collected into EDTA tubes are layered on the surface of this solution. A positive test result is issued when the drop of the effusion stays on the surface, or forms a tailed sinking drop or forms an inverted jelly fish drifting down to the bottom of the test tube (Fischer, Weber et al., 2013). The test result is negative when the drop resolves or the precipitate disappears and the mixture stays clear (Fischer, Weber et al., 2013). Determination of the effusion’s LDH/TNCC ratio might be another feasible tool to decide whether the effusion is FIP associated or not. LDH activity in FIP-associated effusions is usually high despite a low TNCC thus yielding a high fluid LDH/TNCC ratio. In a study including 648 animals, LDH/TNCC ratios > 7.54 increased the probability of an effusion being FIP associated by about 6.59 times (Romanelli et al., 2022). Measuring α1-acid-glycoprotein in feline effusions is also helpful in classifying them as FIP associated; a concentration of >1550 µg/mL yielded a sensitivity and specificity of 93% each ( Hazuchova et al., 2017). Otherwise, viral-induced effusions are rare.

Figure 15.6 Abdominal effusion from a cat infected with FIP virus. Note the large fibrin clot in the sample.
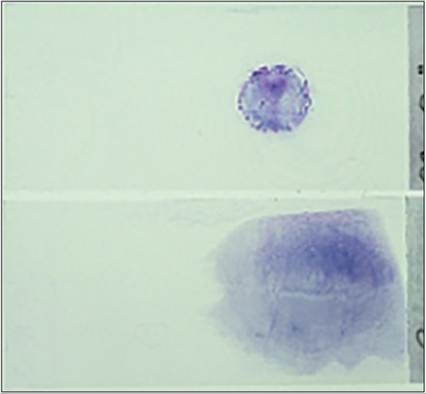
Figure 15.7 Direct smear and cytospin preparation from an effusion from a cat with FIP. The high protein concentration of the effusion results in the gelatinous appearance of the sample.
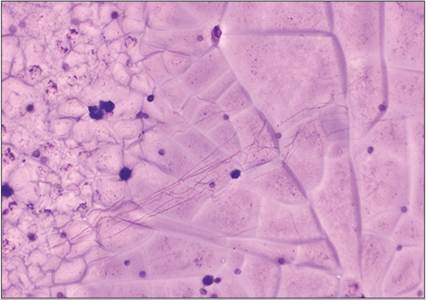
Figure 15.8 FIP virus-associated effusion from a cat. The background is filled with stippled eosinophilic proteinaceous material, so thick that it often appears to have glass-like ‘cracks’ (Hemafix™, 500? magnification).
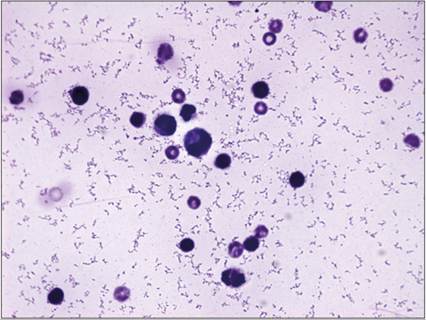
Figure 15.9 FIP virus-associated effusion from a cat. The sample is of low cellularity with few nucleated cells and erythrocytes. The nucleated cells are difficult to evaluate due to the thick proteinaceous background material (Hemafix™, 1,000? magnification).

Figure 15.10 Effusion from a dog. (15.11) The fluid is red and was cytologically consistent with a hemorrhagic effusion. (15.11) Post-centrifugation. Note the red cell pellet and clearing of the supernatant.
Hemorrhagic effusions
An effusion is called hemorrhagic when the effusion is mainly composed of blood (Figures 15.10–15.12). In severe hemorrhage, the composition of the effusion will initially be similar to the animal’s peripheral blood, but will change rapidly due to the reabsorption of fluids, solutes, and cells. Platelets disintegrate and disappear quickly, and fluid will be reabsorbed. Due to fibrinolytic activity of mesothelial cells, a hemorrhagic effusion will not clot when transferred into a native test tube. Reabsorption of fluids occurs more rapidly than absorption of cells, so that the hematocrit of the effusions will soon exceed the hematocrit of peripheral blood. There is no evidence-based fixed threshold for when to address an effusion as hemorrhagic; some authors suggest hemorrhage when the hematocrit of the effusion is more than 25–50% of the hematocrit in peripheral blood (Dempsey & Ewing, 2011; Stockham & Scott, 2013; Epstein & Balsa, 2020); others suggest an RBC concentration above 500 ? 103/µL (Bohn, 2017) or a PCV above 10% (Athanasiou, 2019).
Minor hemorrhage usually accompanies effusions caused by inflammation when vascular permeability is increased. Sampling can cause iatrogenic hemorrhage into a body cavity effusion. Differentiation between iatrogenic and pathologic hemorrhage is important and can be attempted by evaluating the following indicators:
· The clinician taking the sample should be observant if only the first portion of the tap shows bloody discoloration. If so, fractionated sampling should be carried out, where another test tube is filled with the non-bloody fraction of the tap. The non-contaminated fluid is diagnostically more relevant than the first portion.
· Iatrogenic hemorrhagic effusions clot when transferred into a test tube without an anticoagulant. Microscopic evaluation will reveal platelets in traumatic taps, whereas erythrophagocytosis and crystals such as hematoidin (Figure 15.13) and hemosiderin (Figure 15.14), which indicate hemoglobin degradation, are missing. Platelets and platelet clumps usually accumulate in the feathered edge of the smear. As mentioned above, true hemorrhagic effusions do not clot, platelets are usually not visible, and erythrophagocytosis and hemoglobin degradation products can be detected.
· The composition of hemorrhagic effusions changes depending on the cause, amount, frequency, and time course of vascular injury. When frequent minor hemorrhages occur, the oncotic pressure gradient is disrupted with the result that water will spill into the effusion and dilute its content. Hemoglobin will be degraded and form hematoidin or hemosiderin, and macrophages will engulf erythrocytes and/or pigment. Hematoidin crystals (Figure 15.13) are brightly orange rhomboids; hemosiderin appears as blue–green to brown pigment (Figures 15.14, 15.15). Also, when hematopoietic cells are detected in a hemorrhagic abdominal effusion, accidental sampling of the spleen or splenic rupture should be considered.

Figure 15.11 Effusion from a dog. The fluid is red and was cytologically consistent with a hemorrhagic effusion. Post-centrifugation. Note the red cell pellet and clearing of the supernatant.
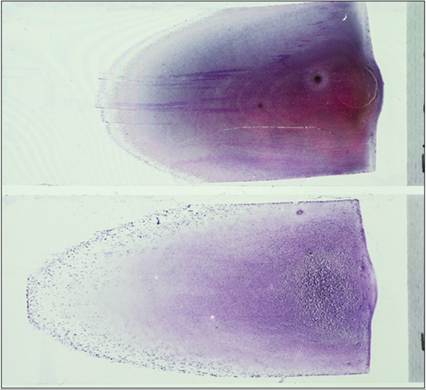
Figure 15.12 Direct smears from two separate effusions. The slide on the top represents a hemorrhagic effusion, the slide below a neoplastic effusion with hemorrhage. The basophilic speckles at the feathered edge likely represent neoplastic clusters of cells.
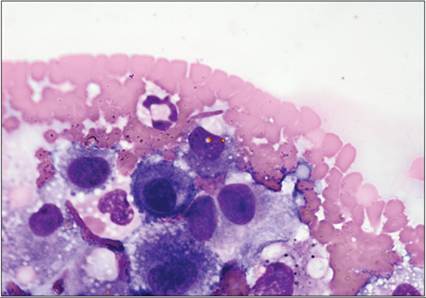
Figure 15.13 Pericardial effusion from a dog. Pictured are macrophages and reactive mesothelial cells and few orange hematoidin crystals (Hemafix™, 1,000? magnification).
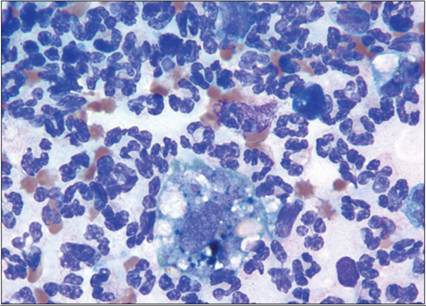
Figure 15.14 Abdominal fluid from a dog. This sample is cellular and consists of neutrophils with a few macrophages. The macrophage pictured contains bluish-green to black pigment consistent with hemosiderin (Hemafix™, 1,000? magnification).
Hemorrhagic effusions can be caused by a variety of events including trauma, coagulation disorders, inflammation, or neoplasia. Packed cell volume and protein content are highly variable depending on the amount and time course of the hemorrhagic event. Acute high volume hemorrhage might result in an effusion in which the hematocrit will be higher than in peripheral blood and will have a high protein concentration. Chronic intermittent bleeding will cause a variable packed cell volume and protein concentration depending on the reabsorption of cells and fluid.
Pericardial effusions are almost always hemorrhagic. Indeed, cytologic evaluation of hemorrhagic pericardial effusion is of limited diagnostic value because it is nondiagnostic in the majority of cases (Cagle et al., 2014). The diagnostic utility was considerably higher when the hematocrit of the fluid was 100 mg/dl (1.13 mmol/l) are defined as chylous (Birchard et al., 1995; Dempsey Ewing, 2011; Valenciano et al., 2013). In recently formed chylous effusions, small lymphocytes are the predominant cell type (Figure 15.18). In chronic cases, neutrophils and macrophages migrate into the effusion and a mixed inflammatory cell population is present (Figure 15.19). Pink, homogeneous, round precipitates of chylomicrons and lipid-filled cytoplasmic vacuoles in macrophages, neutrophils, and lymphocytes are other diagnostic features. Chylomicrons can be stained with Sudan red (Figure 15.20). Chyloabdomen is a rare finding in dogs and cats, but might occur as a symptom of lymphangiectasia in protein-losing enteropathies in dogs. In cats neoplasia was identified as the most common cause for chyloabdomen in a recent study(Hatch, Jandrey et al., 2018). Nonchylous lymphorrhagic effusions occur when nonintestinal lymphatic vessels are affected by hypertension, rupture, or inflammation, food intake has ceased, and/or chylomicrons have been destroyed. The predominant cell type is also the small lymphocyte. Protein concentration in chylous and lymphorrhagic effusion is usually > 2.5 g/dl (25 g/l).
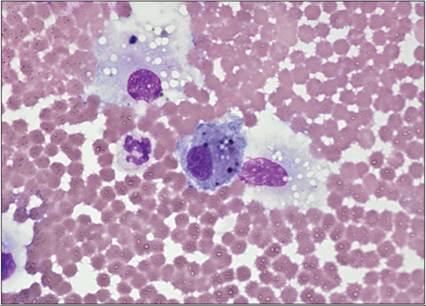
Figure 15.15 Pericardial fluid from a dog. Pictured is a macrophage containing bluish-black pigment consistent with hemosiderin (Hemafix™, 1,000? magnification).

Figure 15.16 Chylous effusion from a cat. The fluid is white and turbid.
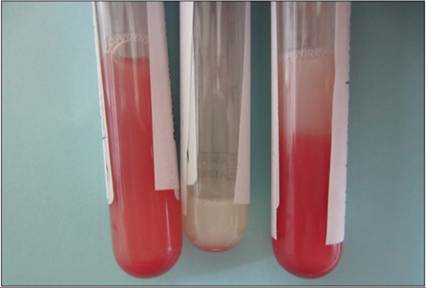
Figure 15.17 Chylous effusion from a cat. This fluid has blood contamination, giving it a ‘strawberry milkshake’ appearance.
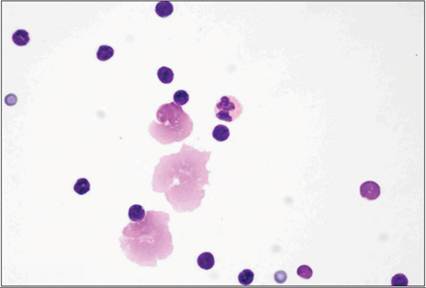
Figure 15.18 Acute chylothorax in a cat. Small lymphocytes predominate. The triglyceride concentration of the fluid was 1,350 mg/dl (15.2 mmol/l) and the cholesterol was 120 mg/dl (1.36 mmol/l) (Hemafix™, 1,000? magnification).
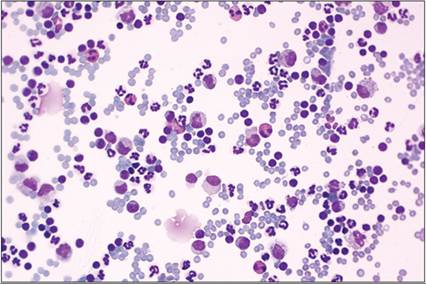
Figure 15.19 Chronic chylothorax in a cat. Small lymphocytes are prominent but a much higher number of neutrophils are present. Vacuolated macrophages are also observed. The triglyceride concentration of the fluid was 1,932 mg/dl (21.8 mmol/l) and the cholesterol 158 mg/dl (1.8 mmol/l) (Hemafix™, 400? magnification).
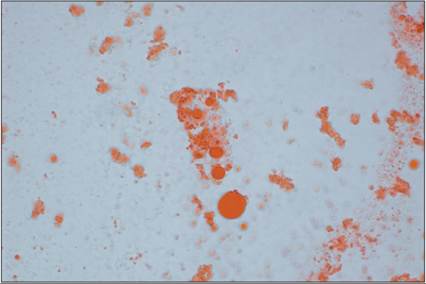
Figure 15.20 Sudan red staining of a chylous effusion can be performed to identify the chylomicrons (Hemafix™, 400? magnification).
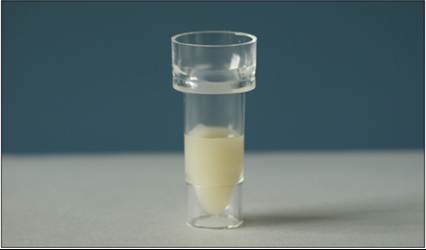
Figure 15.21 Pleural fluid from a pseudochylous effusion. The fluid is white and turbid, similar to a true chylous effusion.
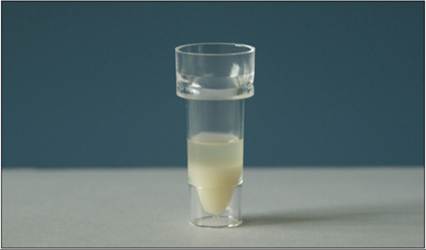
Figure 15.22 Pleural fluid from a pseudochylous effusion. Post-centrifugation. Note the presence of a whitish sediment after centrifugation.
Pseudochylous
Pseudochylous effusions are yellowish to creamy turbid fluids, and no lipid layer forms when the effusion is left standing (Figures 15.21, 15.22). Turbidity is caused by low-density cholesterol-rich lipoproteins. The cholesterol concentration of the fluid exceeds plasma cholesterol concentration, whereas the triglyceride concentration is low. The high cholesterol concentration is caused by disintegrating cell walls being trapped in the body cavity. Cholesterol concentration is much higher in pseudochylous effusions than in plasma. Cellular composition is variable depending on the cause. This type of effusion is not very common in veterinary medicine.
Effusions caused by rupture of a hollow organ or tissue
Uroabdomen
Uroabdomen occurs when urine spills into the abdominal cavity subsequent to trauma, urolithiasis, or neoplasia (Stockham & Scott, 2013). Early uroperitoneum will resemble a transudate unless trauma has caused hemorrhage. Total nucleated cell count and protein concentration are low. Differential cell count will be unaltered in early lesions unless they are caused by neoplasia. Fluid creatinine concentration at least double the plasma creatinine concentration has been applied as a rule of thumb to define uroperitoneum. A recent study suggests a body cavity fluid creatinine concentration ≥2.1 mg/dL (88.42 µmol/L) and a creatininefluid to creatinineserum ratio ≥1.25 as diagnostic cut-offs yielding a diagnostic accuracy of 99% for uroabdomen in dogs (Paes et al., 2022). Eventually, even sterile urine elicits an inflammatory response within the abdominal cavity, so that the protein and cell concentrations may change to an exudate. In suspect cases, comparison between plasma creatinine and fluid creatinine concentration is useful. Determination of urea concentration is less useful, because urea is a small molecule that can diffuse freely, so that it equilibrates much more readily with plasma urea than creatinine. In cases of long-standing uroperitoneum, when the patient is unable to excrete urine, the difference between fluid creatinine concentration and plasma creatinine decreases. If renal function is undisturbed and at least some urine can be voided, the difference remains detectable. Bacteria might be present, if the patient has a concurrent urinary tract infection.
Bile peritonitis
Bile peritonitis occurs when bilious fluid leaks into the abdominal cavity; it can be induced by trauma, inflammation, obstruction, or neoplasia. In rare cases, bile can also leak into the thoracic cavity, for example caused by a fistulous tract from the diaphragmatic surface of the gallbladder (Wustefeld-Janssens et al., 2011). In dogs, the most common cause is a gallbladder rupture due to an undetected and untreated gallbladder mucocele, which is an accumulation of mucus within the gallbladder leading to gallbladder distention and eventual rupture (Thompson & Sherman, 2021). The formation of a mucocele is not completely understood but hypersecretion of mucus from the gallbladder lining epithelium is one of the main mechanisms. The amount of bile lost into the abdominal cavity will not cause a clinically detectable effusion, but due to its irritant properties, bile elicits an inflammatory response. A greenish to brownish, sometimes orange, discoloration of the fluid might give a first hint, followed by microscopic detection of bilirubin crystals or bilious mucus. The diagnosis can be confirmed by comparing fluid and plasma bilirubin concentrations, with fluid bilirubin concentration exceeding plasma concentration. Blood supply for the gallbladder and common bile duct depends on a single artery branching from the proper hepatic artery, making it extremely susceptible to necrosis after trauma (Center, 2009). In cytologic preparations, bilirubin crystals and amorphous blue bilious mucus can be seen (Figures 15.23, 15.24). White bile (representing only mucus secreted by the gallbladder; Figure 15.25) is encountered when bile pigment is trapped within liver parenchyma during cholestatic disease and gallbladder content oozes into the abdominal cavity.
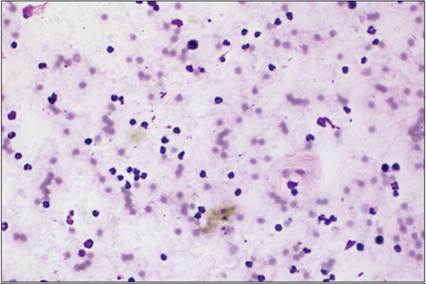
Figure 15.23 Abdominal fluid from a dog. The sample is cellular. Direct smears reveal a smudged background consisting of red blood cells, pyknotic cells, neutrophils, and pigmented precipitate (Hemafix™, 400? magnification).
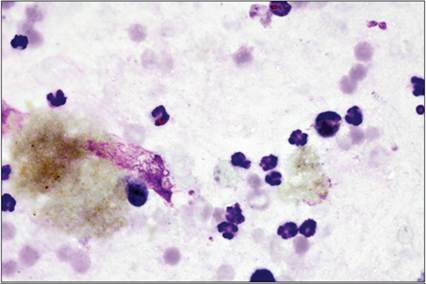
Figure 15.24 Abdominal fluid from a dog. Aggregates of greenish-gold pigmented material consistent with bile (Hemafix™, 1,000? magnification).
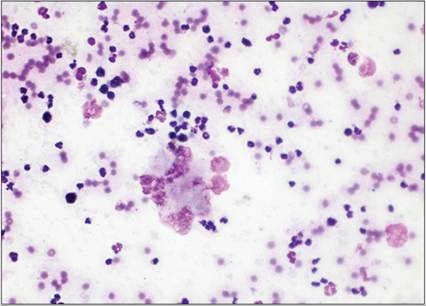
Figure 15.25 Direct smear from bile peritonitis from a dog. The sample is cellular and consists of neutrophils with a smudged background, pink mucinous material, or ‘white bile’ (Hemafix™, 400? magnification).
Leakage of gastric or intestinal contents
Leakage of gastric or intestinal contents might be caused by foreign bodies, ischemia, severe gastrointestinal inflammatory disease, or neoplasia. Again, the amount of material leaking into the body cavity might be negligible, but it will induce a severe inflammatory response and cause a septic exudate. Leakage of chyme influences the gross appearance of the fluid, causing changes in color, odor, and viscosity. Food particles might be detected by gross examination but also by microscopy (Figure 15.26). A mixed bacterial population is typical for secondary septic peritonitis.
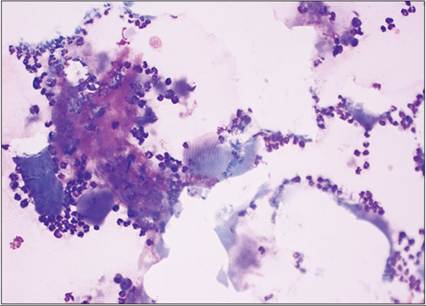
Figure 15.26 Abdominal fluid from a dog with a penetrating foreign body. Striated skeletal muscle is observed (Hemafix™, 400? magnification).
Neoplastic effusions
Tumor-associated effusions
Tumor-associated effusions show a high variability in their composition. An effusion is classified as tumor associated when tumor cells can be identified during microscopic examination. However, not all tumor-associated effusions yield a sufficient number of tumor cells; therefore complementary diagnostic imaging is needed to establish a diagnosis. Tumors might cause transudation by obstructing venous or lymphatic drainage; they can elicit exudation by inciting an inflammatory reaction or rupture of an internal organ or cause hemorrhage, or a combination of those mechanisms. Cytology is an excellent but not overall sensitive tool to identify tumor-associated effusions. Sensitivity and specificity of cytology were 65% and 99%, respectively, for dogs and 61% and 100% for cats (Hirschberger et al., 1999). In severely hemorrhagic effusion the diagnostic sensitivity for detecting neoplastic cells is considered low (Cagle et al., 2014). Diagnosis is facilitated when tumor cells exfoliate into the effusion and can be differentiated from reactive mesothelial cells, but absence of tumor cells does not rule out neoplasia. Detection of a mass by diagnostic imaging and directly obtaining a sample from the lesion might be a more efficient approach. Determination of the origin of neoplastic cells with Romanowsky-type stains is often difficult and has to be complemented by special stains. Reactive mesothelial cells are especially difficult to differentiate from epithelial neoplasia, as they also show criteria of malignancy as indicators of proliferative activity in terms of healing or inflammatory stimulation. As always, severe inflammation is a complicating factor in the interpretation of cytopathologic criteria of malignancy. However, cytology is still an excellent tool in identifying neoplastic effusions (Hirschberger et al., 1999). Special cytochemical stains for identifying tissue-specific intermediate filaments, such as cytokeratin, vimentin, and desmin, are useful for establishing a definitive diagnosis. Cytologic preparations are stable at room temperature for at least 24 hours prior to staining (Przeździecki & Sapierzyński, 2013). Preparation of cell blocks from effusions is a feasible alternative to preserve effusion-derived cells for additional cytochemical staining, thus aiding the identification of cells (Melega et al., 2020).
Lymphoma-associated effusions
Lymphoma-associated effusions are relatively common when internal lymph nodes or organs are affected. Microscopic evaluation reveals a variable number of immature lymphoid round cells. Small-cell lymphoma might be difficult to diagnose by cytology alone, so complementary diagnostic testing, such as clonality testing by polymerase chain reaction, is warranted. When cell concentrations are determined by advanced laser-based flow cytometry, characteristic cytograms are generated, which have to be confirmed by microscopic evaluation (Figures 15.27–15.30) (Bauer & Moritz, 2005).
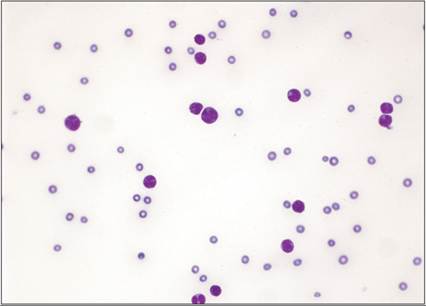
Figure 15.27 Pleural fluid from a dog with a mediastinal mass. Large round cells are observed with round to occasionally lobulated nuclei and smooth chromatin. The mass is a lymphoma (Hemafix™, 400? magnification).
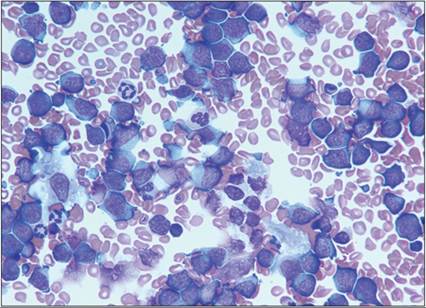
Figure 15.28 Pleural fluid from a dog with lymphoma: cytospin preparation. The sample consists of a population of large lymphocytes. These cells are round with a scant rim of basophilic cytoplasm and large prominent nucleoli (Hemafix™, 1,000? magnification).
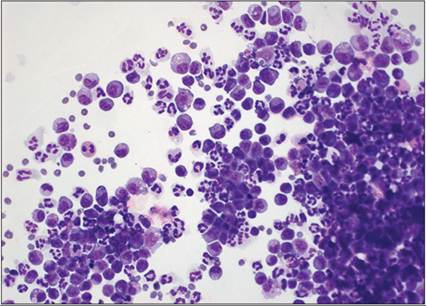
Figure 15.29 Abdominal fluid from a cat with large granular cell lymphoma. There is a population of large round cells containing variable numbers of pink cytoplasmic granules. The nuclei are round with prominent nucleoli (Hemafix™, 400? magnification).
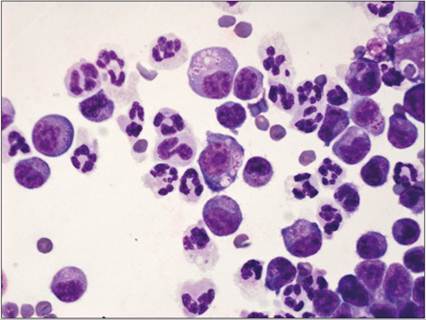
Figure 15.30 Abdominal fluid from a cat with large granular cell lymphoma. The granulation is quite prominent in some cells and the granules are variably sized (Hemafix™, 1,000? magnification).
Mast cell tumor
Mast cell-associated effusions are more common in cats than in dogs because in this species internal organs are more often affected by mast cell tumors (Valenciano et al., 2013). Mast cells exfoliate readily into the effusion and can be identified by their variable content of magenta to purple colored granules (Figures 15.31–15.35). As in other lesions, mast cells in effusions can be accompanied by eosinophilia.
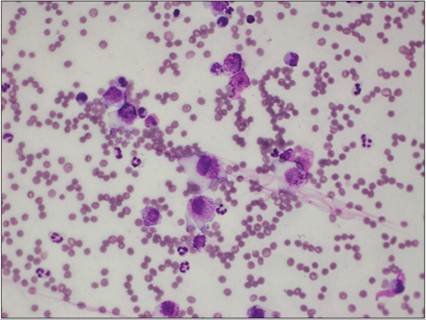
Figure 15.31 Abdominal fluid from a dog with mast cell neoplasia. Variably sized mast cells are observed (Hemafix™, 400? magnification).
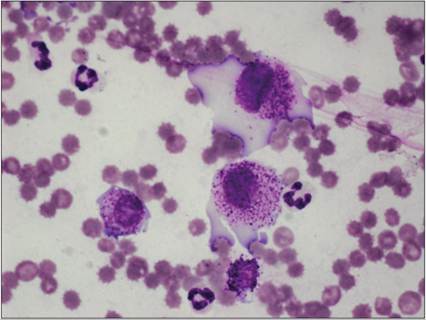
Figure 15.32 Abdominal fluid from a dog with mast cell neoplasia. Because of the intermediate amount of granulation, nuclear features can be easily evaluated and include anisokaryosis and prominent, irregular nucleoli (Hemafix™, 1,000? magnification).
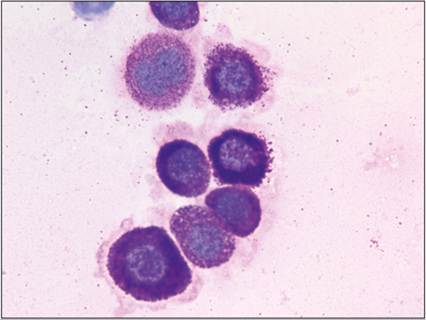
Figure 15.33 Cytospin preparation from abdominal fluid from a dog with visceral mast cell neoplasia (Hemafix™, 1,000? magnification).
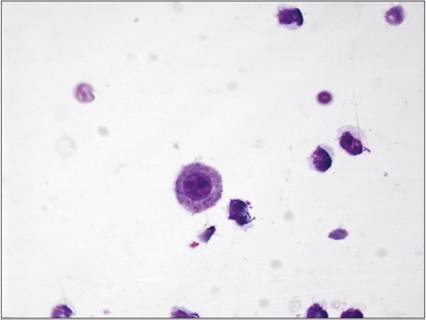
Figure 15.34 Abdominal fluid from a dog with splenic masses. The fluid is of low cellularity. Poorly differentiated mast cells with minimal granulation can be difficult to identify (Hemafix™, 1,000? magnification).
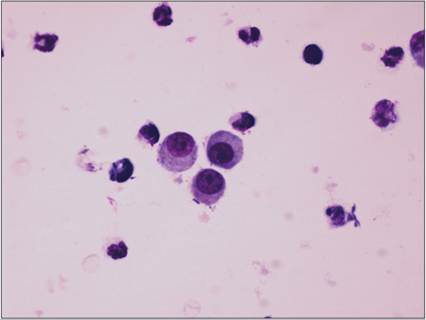
Figure 15.35 Abdominal fluid from a dog with splenic masses. Round cells are observed; only the cell on the left has a few tiny metachromatic granules (Hemafix™, 1,000? magnification).
Other round cell tumors
Other round cell tumors, such as multiple myeloma (Figures 15.36, 15.37) or malignant histiocytosis (Figures 15.38, 15.39), might also exfoliate into body cavity effusions, thus indicating the etiology.
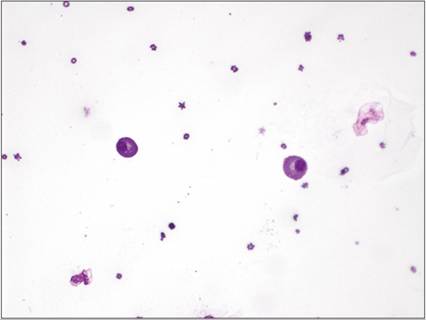
Figure 15.36 Pleural fluid from a cat with multiple myeloma. Well-differentiated plasma cells are identified with eccentrically located nuclei and perinuclear clear areas. The total protein in the effusion was 7.5 g/dl (75 g/l) (Hemafix™, 400? magnification).
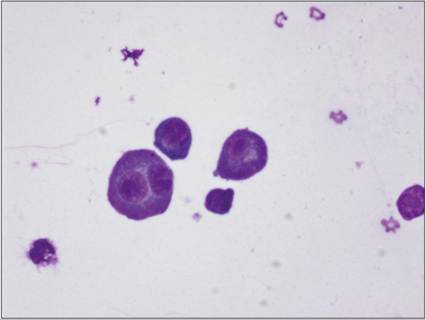
Figure 15.37 Pleural fluid from a cat with multiple myeloma. Atypical plasma cells are also noted, with binucleation and prominent, irregular nucleoli (Hemafix™, 1,000? magnification).
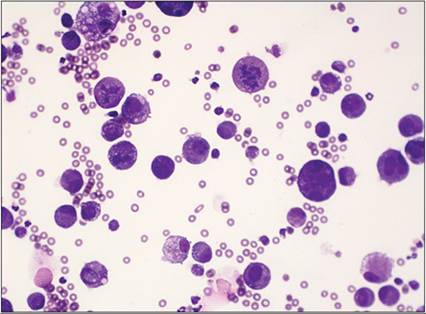
Figure 15.38 Abdominal fluid from a Bernese Mountain Dog with histiocytic neoplasia. The sample is cellular and consists of a population of large neoplastic round cells. Anisocytosis, anisokaryosis, and atypical mitotic figures are observed (Hemafix™, 400? magnification).
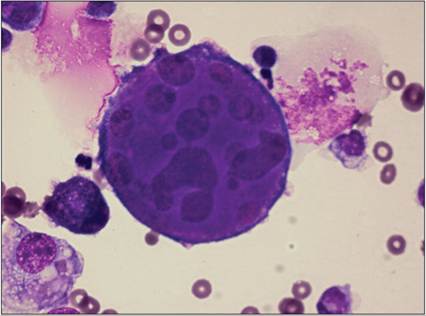
Figure 15.39 Abdominal fluid from a Bernese Mountain Dog with histiocytic neoplasia. Marked atypia is observed in this sample, with bizarre ballooning giant cells, anisokaryosis, and irregular nucleoli (Hemafix™, 1,000? magnification).
Sarcomas
Sarcomas such as hemangiosarcoma are not easily detected by cytologic evaluation of body cavity effusions as they do not exfoliate well. Rupture of the tumor and formation of a hemorrhagic effusion raise suspicion; however, even tumor rupture does not yield a high number of tumor cells in the effusion. Inspection of the feathered edge or buffy coat preparations increases the sensitivity for detection of mesenchymal tumor cells (Figures 15.40, 15.41) (Valenciano et al., 2013). Detection of canine prostate specific membrane antigen (cPMSA), which is expressed by endothelial cells in canine hemangiosarcomas, in hemorrhagic effusions might help to establish a final diagnosis of this tumor type (Dowling et al., 2019).
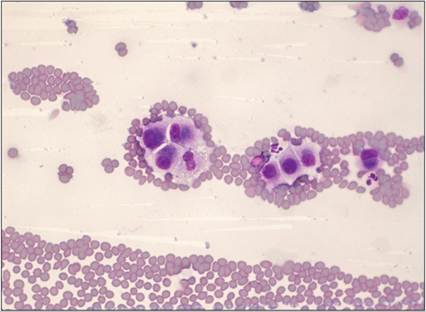
Figure 15.40 Pericardial effusion from a dog with hemangiosarcoma. Low numbers of pleomorphic plump mesenchymal cells are noted (Hemafix™, 400? magnification).
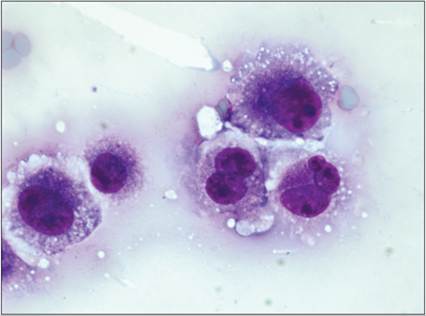
Figure 15.41 Pericardial effusion from a dog with hemangiosarcoma. The nuclei contain prominent irregular nucleoli. Variation in the nucleoli is observed (Hemafix™, 1,000? magnification).
Mesotheliomas
Mesotheliomas (Figures 15.42–15.44) are uncommon tumors in small animals and, as mentioned above, difficult to differentiate from carcinoma or adenocarcinoma (Valenciano et al., 2013). Development of these tumors has been associated with exposure to asbestos, aluminum oxide, or simian virus 40, and in young animals, where congenital forms seem to exist (Martins et al., 2011). The identification of a primary tumor by diagnostic imaging might suggest carcinoma or adenocarcinoma. Otherwise, immunohistochemistry is useful to distinguish between carcinomas/adenocarcinomas and mesothelioma (Reggeti et al., 2005; Bacci et al., 2006; Al-Dissi & Philibert, 2011). Mesothelial cells stain positive for cytokeratin, vimentin, and desmin, defining a characteristic pattern for cells of mesothelial origin (Przeździecki & Sapierzyński, 2013). Double staining protocols for Romanowsky stained slides with Wilms-tumor antigen (WT-1) and cytokeratin to identify reactive mesothelial cells are useful in differentiating them from carcinoma cells (Marrinhas et al., 2022). By histopathology, the differentiation of epithelioid from mesenchymal types of mesothelioma and mixed types can be achieved (Valenciano et al., 2013). Electron microscopy might be another useful tool in establishing a diagnosis of mesothelioma. Mesothelial cells have unique long, often branching, microvilli, a continuous basement membrane, and prominent desmosomes that can be visualized by that technique (Bacci et al., 2006; Al-Dissi & Philibert, 2011). Diagnosis of mesothelioma by cytology alone is discussed controversially yielding a highly variable sensitivity from 4 to 77% (Milne et al., 2021). Immunohistochemistry on cell block preparations is useful in differentiating mesothelial hyperplasia, mesothelioma, and carcinoma in dogs when compared with biopsy results (Milne et al., 2021). A panel of cytokeratin, WT-1, desmin, and m-RNA binding protein 3 (IMP3) appeared to be most useful in distinguishing reactive mesothelial cells, mesothelioma, and carcinoma (Milne et al., 2021).
Figures 15.42 Pleural fluid from a Bernese Mountain Dog with malignant mesothelioma. A cluster of neoplastic cells exhibiting basophilic cytoplasm and in other cells ballooning pink cytoplasm, large nuclei with coarse chromatin. Mesothelioma was confirmed at necropsy (Hemafix™, 1,000? magnification).
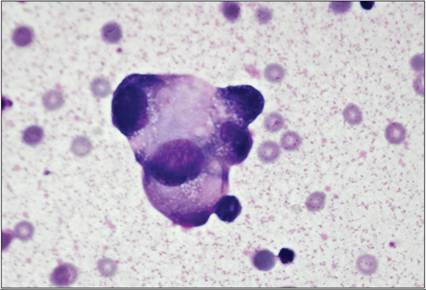
Figure 15.43 Pleural fluid from a Bernese Mountain Dog with malignant mesothelioma. Bizarre ballooning cells, marked anisocytosis and anisokaryosis, and macronuclei with inconspicuous nuclei (Hemafix™, 1,000? magnification).
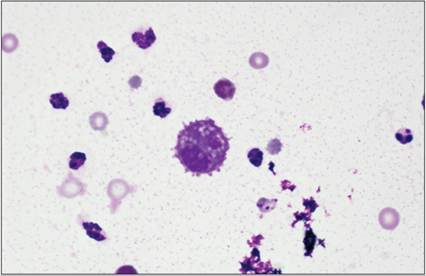
Figure 15.44 Pleural fluid from a Bernese Mountain Dog with malignant mesothelioma. Note the single mesothelial cell arranged in a background of thick stippled proteinaceous material (Hemafix™, 1,000? magnification).
Carcinomas and adenocarcinomas
Carcinomas and adenocarcinomas exfoliate in clusters (Figures 15.45–15.51). Demonstration of strong nuclear criteria of malignancy should elicit diagnostic imaging to identify an eventual primary tumor, which can be accessed for fine needle aspiration (Valenciano et al., 2013). Cytologic evaluation of the effusion alone cannot reliably identify the tissue of origin. Thus, immunocytochemistry is useful to classify the cells as epithelial by a positive staining for cytokeratin.
Figures 15.45 Pleural fluid from a dog with a history of a primary lung carcinoma. Clusters and individualized epithelial cells are observed. The individualized cells have ballooning cytoplasm and one cell has a signet ring appearance (Hemafix™, 400? magnification).
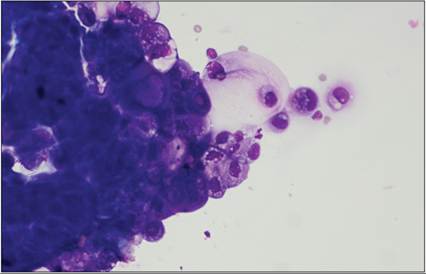
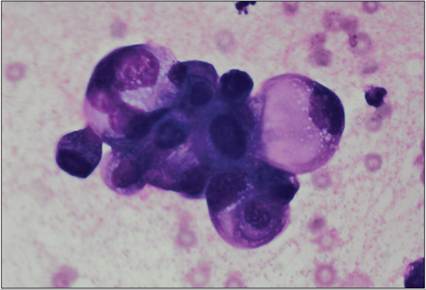
Figure 15.46 Pleural fluid from a dog with a history of a primary lung carcinoma. A large cluster of irregular epithelial cells exhibiting marked anisocytosis, anisokaryosis, perinuclear vacuolization, and occasionally ballooning cytoplasm are pictured (Hemafix™, 400? magnification).
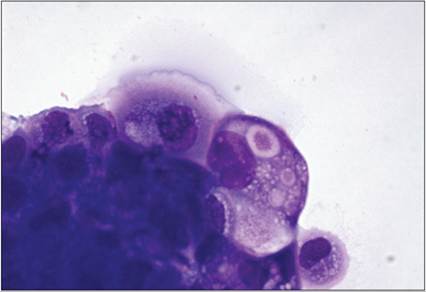
Figure 15.47 Pleural fluid from a dog with a history of a primary lung carcinoma. Higher magnification. The cytoplasm contains eosinophilic granular to globular material. Prominent nucleoli are visualized (Hemafix™, 1,000? magnification).
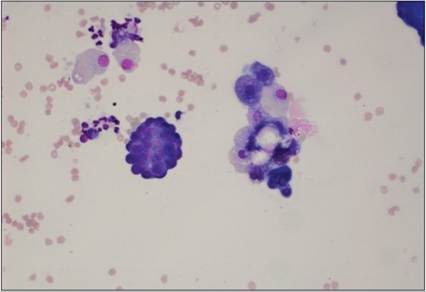
Figure 15.48 Abdominal fluid from a Yorkshire Terrier with a history of ovarian carcinoma. Dense clusters of neoplastic epithelial cells are observed, occasionally exhibiting a papillary cluster (Hemafix™, 200? magnification).
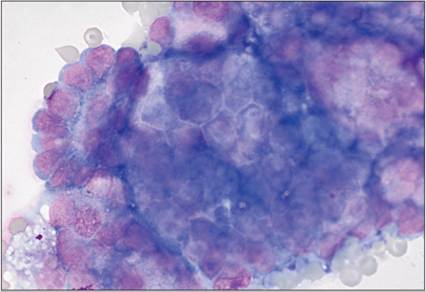
Figure 15.49 Abdominal fluid from a Yorkshire Terrier with a history of ovarian carcinoma. Higher magnification revealing a globoid cohesive epithelial cluster exhibiting anisocytosis and anisokaryosis (Hemafix™, 1,000? magnification).
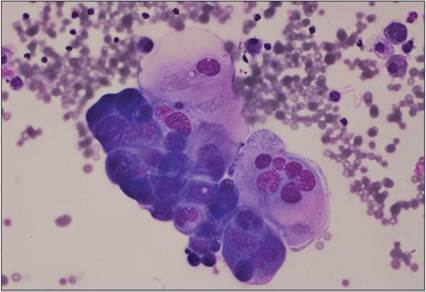
Figure 15.50 Abdominal fluid from a dog with prostatic carcinoma. A cluster of cells with multinucleation and marked anisocytosis and anisokaryosis are observed (Hemafix™, 400? magnification).
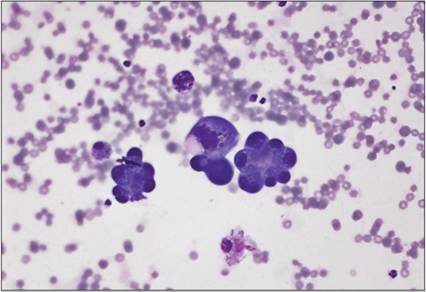
Figure 15.51 Abdominal fluid from a dog with prostatic carcinoma. Acinar structures are observed with a multinucleated cell (Hemafix™, 400? magnification).