THE DIGESTIVE TRACT
The Teeth
Cattle have front teeth, or incisors, only in their lower jaw (Figure 13.1). They pull grass into their mouth using their tongue and then cut it off by closing the incisors against the upper gums.
Calves are born with eight temporary incisors and these are replaced at a later date by permanent teeth. As in children, the central pair of incisors is replaced first, and the number of permanent teeth present at any one time can be used to age the animal. The approximate ages of eruption are given in Table 13.1Examination of dentition became very important following the UK BSE crisis in the 1990s, because animals over 30 months old were not allowed to enter the human food chain. However, this demonstrated the inaccuracy of ageing, because there were plenty of animals over 30 months old with only two teeth showing and, conversely, plenty under 30 months old with three or four teeth!
The teeth come into wear approximately three months after eruption, so that a heifer is almost four years old before she is using her full set of permanent incisors. The table also shows that a two year old calving heifer will have to change almost all her teeth during her first lactation and this is bound to cause problems with feeding (Plate 13.1). For example if self-fed from a heavily compacted silage face 3 m high, young growing and finishing animals can be affected by weight loss, presumably because they are changing their teeth. One trial in Ireland showed a reduction in weight gain of 0.27 kg/day comparing selffeed silage with easy feed.
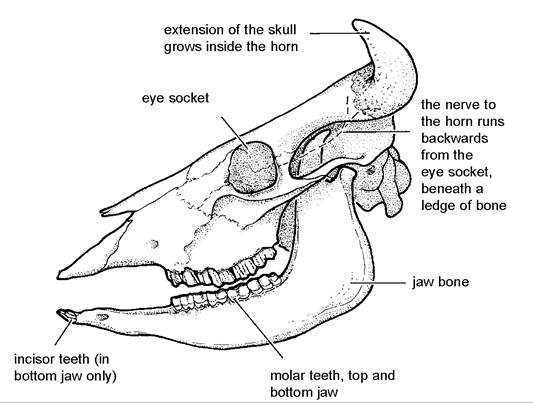
Figure 13.1. The skull of a cow. Note that there are front (incisor) teeth in the lower jaw only.
Table 13.1. The approximate age at which the permanent incisors erupt.
| Incisor teeth | Age of eruption |
| Central pair | 1 year 9 months (21 months) |
| Second pair | 2 years 6 months (30 months) |
| Third pair | 3 years (36 months) |
| Outer pair | 3 years 6 months (42 months) |
There are three temporary molars, or grinding teeth, on each side of the upper and lower jaws.
These are replaced by six permanent molars, so that the adult cow has a total complement of 32 teeth (four sets of six molars plus eight incisors). The permanent teeth grow throughout adult life and the incisors change from a spade shape in a young cow to small square pegs in the aged animal (Figure 13.2).
Plate 13.1. A heifer changing her teeth. While the teeth are loose like this she will find eating more difficult, especially from a compacted self-feed silage face.
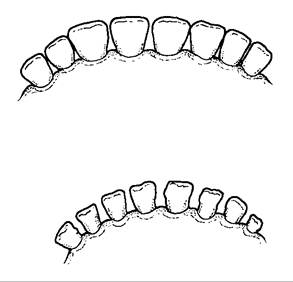
Figure 13.2. Incisors change with age from a spade shape to small pegs in the old cow.

Plate 13.2. Fractured jaw in a calf. Put back onto milk, the calf healed without treatment.
Tooth abscesses
These are uncommon but should always be looked for in a drooling animal. The incisors are most commonly affected and often cause a swelling of the lower lip. Most respond to antibiotic treatment.
Fracture of the jaw
Provided that the fracture occurs at the symphysis, which is the natural join of the two jaw bones under the incisor teeth, most animals recover well without treatment. The calf in Plate 13.2 was put back onto milk, to make feeding easier, and made a full recovery.
Misaligned molars
This most commonly occurs as a result of a lumpy jaw bone infection (see Chapter 10). There is no useful treatment.
Undershotjaw
During feeding it is necessary for the teeth to make contact with the hard palate, in order to achieve a cutting action. If the bottom jaw is too short (Plate 13.3), the incisor teeth fail to make good contact with the gums and eating becomes difficult. The 18 month old heifer shown in Plate 13.3 was much smaller than the rest of her group. There is no treatment.
Severe incisor wear
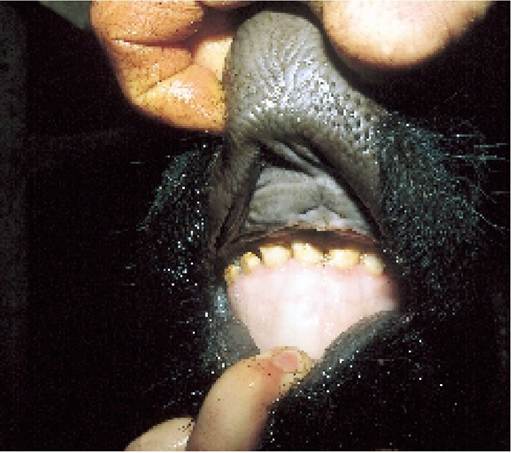
Plate 13.3.
An undershot jaw. This 18-month-old heifer remained stunted because she was unable to feed properly.In some cows the incisor teeth become so badly worn that it seriously affects their ability to eat. If the teeth are so badly eroded that the dentine (quick) is exposed, eating will be particularly painful. Food intake falls and weight loss occurs.
Very acid silage has been suggested as a cause of severe incisor wear. However, although extracted teeth become pitted if exposed to very acid silage, the high pH of saliva in the mouth probably counteracts any effect of silage acid in the living animal.
Jaw abscesses, wooden tongue, lumpy jaw, malignant oedema and blaine are described in Chapter 10.
Choke
Moving away from the mouth and down into the oesophagus, the main problem here is an obstruction and the animal is said to have choke. Potatoes and apples are most commonly involved and they are considered particularly dangerous if apples are eaten from trees or if potatoes are eaten from raised troughs. This is because when the animal eats food from the ground, it is more likely to be chewed into small pieces before it is swallowed.
Clinical signs
The first indication that there is something wrong may simply be that one animal is standing apart from the others, with its head stretched forwards and its mouth slightly open. It may go up to feed, but then turns away again. If the blockage is severe, saliva produced in the mouth cannot be swallowed and so the animal will be drooling. On the other hand, gas cannot escape from the rumen and bloat develops. If left untreated, there is a risk of death either from severe bloat or from infection due to an erosion of the oesophagus at the point of obstruction.
Treatment
Saliva and digestive juices from the mouth often dissolve enough of the potato or apple for the remainder of it to be swallowed and some people say that the best treatment is to insert a trocar and cannula (Plate 13.8 and Figure 3.2) into the rumen to alleviate bloat and then leave the animal to recover on its own.
Drugs are available which help to relax and dilate the oesophagus, thereby making it easier for the foreign body to pass down into the rumen.Alternatively you can try to push the obstruction down into the rumen using a probang. This is a long length of pliable nylon tubing with an enlarged metal lump at one end. The handle is attached to a long cane which runs through the centre of the tube to give added rigidity. The animal’s mouth is held open using a metal gag (Plate
13.4) inserted between the teeth, and the probang is carefully pushed down the oesophagus. If you push too hard there is a danger that you will rupture the wall of the oesophagus, so this is a job which is best left to your vet.
The best treatment, but sometimes not possible, is to work the potato up the oesophagus from outside and then, with a gag in position, push your hand into the animal’s mouth and pull the apple out. This was successfully achieved with the calf in Plates 13.5 and 13.6. Sometimes you have to wait for a few hours (or even days) for the oesophagus to relax sufficiently and/or for the apple to be digested enough to be able to achieve this.
Never put your hand into the back of an animal’s mouth without using a gag (Plate
13.4). The molar teeth are strong enough to cut off your finger - a near miss is shown in Plate 9.20B!
Vomiting
Cows rarely vomit. If they do, it could be due to:
• wooden tongue (Chapter 10) at the base of the oesophagus, that is where it enters the rumen. A five to seven day course of antibiotics by injection may help to resolve this
• acidosis, causing the cud to be regurgitated (see page 397)
• rhododendron poisoning (page 450)
Bloat (Ruminal Tympany)
Gas is produced by the micro-organisms in the rumen as part of the normal fermentation of food; following a meal the rate of gas production may be as much as 30 litres per hour. If it cannot escape, it makes the rumen

Plate 13.4.
The mouth gag slots over the top and bottom molar teeth and in so doing holds the mouth open.
Plate 13.5. Choke: the foreign body in the oesophagus can be seen just above the operator’s hand.

Plate 13.6. Choke: this was a fortunate case in which the apple could be squeezed up, into and out of the animal’s mouth. Note how the outside of the apple has undergone digestion by the salivary enzymes.
swell and this we call bloat. The rumen is situated on the left side of the animal, so that bloat is first seen as a swelling in the left flank, as in the calf in Plate 2.15. In more advanced cases, however, both sides will be distended. The animal is obviously in discomfort by now and it stands stiffly, with its legs spread wide apart. A typical example is shown in the calf in Plate 13.7. It may be drooling or frothing at the mouth and if you examine it carefully you will find that the heart is beating extremely rapidly. Eventually the pressure inside the rumen becomes so great that the animal goes down onto its side and death soon follows, either from heart failure or because liquid rumen contents have been forced up into the throat and inhaled into the trachea.
To appreciate how bloat develops it is important to understand how the normal rumen functions. The ruminant has four stomachs as follows.
The rumen is a large fermentation vat (approximately 200 litres in an adult cow) where micro-organisms (bacteria and protozoa) ferment ingested food at around pH 6.5 and in the absence of air. The length of time the food stays in the rumen varies with the type of food and the amount eaten. It can take up to ten days for it to be broken down through fermentation and chewing the cud into small enough particles to pass on. However, this is an extreme example. An average forage will be retained in the rumen fibre mat (Figure 13.3) for around thirty hours, and concentrates, which are broken down quite rapidly, for as little as ten hours.
Products of fermentation, absorbed from the rumen into the blood, are used as food by the cow.The reticulum is really an additional part of the rumen. Contractions help to force small food particles into the omasum. The heavy autoworm (Figure 4.5) and trace element boluses are retained in the reticulum, as are other ingested metallic objects, some of which may later penetrate to produce the classic ‘wire’ (Figure 13.3).
The omasum's main functions are the absorption of water (about half the total water drunk is absorbed here) and rumen fermentation products. It also prevents the reflux of food back from the abomasum into the rumen.
The abomasum is the ‘true’ stomach, with a very acid pH of 1-2. Its digestive enzymes and functions (see Chapter 2) are similar to those of the human stomach.
There are approximately two waves of rumen muscle contraction each minute. In the first wave

Plate 13.7. Severe bloat. Both sides of the abdomen are dilated. The heifer has her head down and legs apart, attempting to remain standing.
The four stomachs of the ruminant:
• the rumen
• the reticulum
• the omasum
• the abomasum
The rumen, reticulum and omasum together are sometimes referred to as the forestomachs.
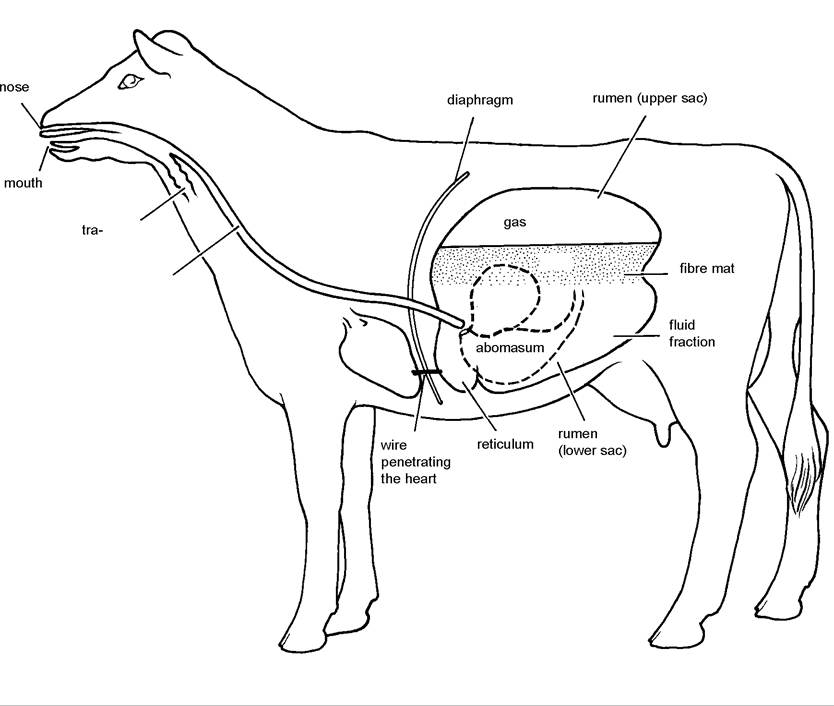
Figure 13.3. Upper digestive tract of the cow showing the point at which a wire penetrates the reticulum and its close proximity to the heart.
the lower sac of the rumen and the reticulum contract: this mixes the food, and any liquid sludge which has finished its digestion is transferred into the omasum, the third stomach (see Figure 13.3). During the second wave of muscular contraction, the upper sac of the rumen compresses the gas, forcing it down towards the reticular end of the oesophagus, which then opens to allow the gas to escape into the mouth.
Fibrous food is also transferred back to the mouth for further chewing by the same process, known as eructation, and we say that the cow is ‘chewing her cud’. An essential part of any examination of a cow’s health is to stand back and watch to see if her rumen is functioning correctly. It is easy to see the left flank moving in and out as the rumen contracts twice each minute, and eructation with regurgitation is clearly audible.
Causes of bloat
Bloat occurs when something interferes with the natural processes of gas release. This can occur in three ways: first a lack of ruminal contractions, second an obstruction in the oesophagus and third the presence of froth or foam in the rumen. Causes of bloat are listed in Appendix 2.
Cessation of ruminal contractions This is technically called ruminal ‘atony’. It occurs most commonly in the weaned calf and the symptoms and treatment were discussed in Chapter 3. Atony is also seen as part of the vagus indigestion complex in adult cows, when the nerve supply to the rumen has been damaged; in association with acidosis, e.g. caused by grain overload, where it may be referred to as feedlot bloat (page 170); and secondary to other conditions such as a wire, overeating of potatoes and digestive upsets. Failure of rumen contractions can occur with tetanus (Chapter 4) or botulism (Chapter 4) and may also cause bloat.
Obstruction in the oesophagus Choke is the most common obstruction, although abscesses and occasionally tumours (for example EBL, Chapter 11) compressing the outside of the oesophagus can cause a blockage. Actinobacillosis infection (wooden tongue) of the lower end of oesophagus can cause bloat or regurgitation of food (vomiting): a five to seven day course of antibiotics should effect a cure.
Frothy bloat Normally free gas collects as a single bubble in the upper part of the rumen (Figure 13.3) until it is expelled. However, under certain conditions, as the gas is released from the semi-solid fermenting food in the bottom of the rumen it forms a froth or foam. This foam can be very stable, so much so that the gas it contains cannot be expelled by the normal mechanisms of ruminal contraction, so although the rumen is contracting and there is no obstruction in the oesophagus, a severe and often fatal bloat develops.
Certain pastures are particularly prone to producing frothy bloat. For example, alfalfa can be a problem and animals may become bloated and die only ten to fifteen minutes after they have started grazing. In Britain, clovers, lush leys and even kale are more commonly involved. It seems to be the stage of growth rather than the species of plant or weight of crop which is important. If you find that you are getting several blown cows in a particular field, simply take them away for two to three weeks. After this period the same pasture may be quite safe to graze again, even though the crop may then be even heavier.
Treatment
Whatever is causing the bloat, the prime objective of treatment must be to relieve the pressure of the gas before it leads to heart failure. You may not know which type of bloat you are dealing with, so, provided that the animal is only moderately affected, first take it out of the field if it is grazing, and give it a bloat drench. This is something which you should always have in stock, ‘just in case’. If you do not have any, then 500 ml of linseed oil works well for a cow. If she is unable to swallow the drench, then you know you are dealing with an obstruction and you need to call for veterinary assistance. Bloat drenches (including linseed oil, poloxalene and other surfactants) act by dispersing the foam. Free gas can then be expelled in the normal way. You may even hear the cow belch within a few minutes of giving the drench and then you know that all is well.
The safest way of releasing the gas, provided the cow is still standing, is to pass a stomach tube. Hold the cow’s teeth apart using a gag (Plate 13.4) and push a length of fairly soft 20 mm plastic tubing into the throat. As you feel her swallow, push the pipe slightly further and then down into the oesophagus. If this produces a cough, or if you can feel air rushing in and out of the end of the pipe as the animal breathes, you know that you are in the trachea and you must start again. I find stomach tubing works well in younger cattle, but it is less successful in adults, partly because the end of the pipe gets caught in the food and liquid at the bottom of the rumen (Figure 13.3) and so the gas is not released. If this happens, move the tube in and out of the rumen until you get to a position where gas flows. Sometimes it helps to blow down the tube: this will often remove the obstruction, more gas flows until it blocks and then you can blow again. Whether you are using a trocar and cannula or a stomach tube, if frothy bloat is present the foam will probably be so stable that it will not pass out and this is why a froth-dispersing drench should always be given first.
It is important to keep a bloated animal on its feet for as long as possible and this is why traditionally they were walked for long periods. Once the cow lies down you have an extreme emergency on your hands because death follows quite quickly. Try to get her to stand up again so that you can give her a
bloat drench. If this is not possible, or if it has not worked, you must release the gas, preferably using a trocar and cannula. The trocar, which has a handle at one end and a sharp metal point at the other (Plate 13.8), fits inside the cannula. It will need to be held in both hands like a dagger and brought down with tremendous force to penetrate the skin of the cow. Once in the rumen, remove the trocar so that gas can escape through the cannula. Hold the cannula in position while the gas is escaping, then call for veterinary assistance to have it sutured in position. If the rumen slips off the end of the cannula while gas is escaping, rumen contents will be discharged into the abdomen and this could lead to severe peritonitis and even death.
If you do not have a trocar and cannula, then in an extreme case a large carving knife with a wide blade can be used. Push the knife into the rumen, then turn the blade through 90 degrees and hold it transversely across the original cut, so that the gas can escape. The correct position to puncture and deflate a cow is shown in Figure 3.2 and Plate 13.9. It is on the left side, 5 cm behind the last rib and 15 cm down from the spine.
I should stress that releasing the gas in this way should only be done as an extreme measure and only when the cow is recumbent. There is a
Plate 13.8. Atrocar and cannula. The trocar has a sharp point to enable it to be forced through the skin and into the rumen. The holes in the collar around the base of the cannula allow it to be sutured into position when the trocar has been removed.


Plate 13.9. In severe bloat a trocar and cannula can be forced through the skin on the left flank.
serious risk of peritonitis and other
complications which can be fatal to the cow, especially if a carving knife is used. In either case, you
should call your vet to advise you on how to dress the wound and to give any other antibiotic treatment
necessary to prevent peritonitis.
Prevention
Cows grazing lush pasture should always be given access to mature silage, hay or palatable straw before turnout. Not only does this reduce the incidence of bloat, but it also helps to maintain butterfat (see Chapter 6), reduces the incidence of hypomagnesaemia and helps to prevent ruminal impaction and the ‘cold cow’ syndrome. If you are forced to graze bloat-producing pastures, they can either be sprayed daily with mineral oils, or a better alternative is to add the chemical poloxalene or other surfactants to the drinking water, using a proportioner similar to that shown in Figure 6.5, or include it in the concentrate. The drinking water route is preferred, because supplementation can be installed very quickly and all cows must drink, whereas many of them may not be receiving concentrate when they are grazing lush pasture. Poloxalene can also be used very effectively as a bloat drench, that is, for treatment.
Overeating Syndrome (Acidosis)
Another condition which primarily involves the rumen and which can affect cattle of all ages is the overeating syndrome. This is most commonly seen when a door to a concentrate or grain store has been blown open, or possibly some sacks of concentrate have been left within reach of the cows. Sometimes a group of calves is accidentally given double their normal ration and a few gorge themselves.
Once in the rumen the grain is rapidly fermented by the bacteria. This produces very acid conditions (lactic acid) and, if severe, contractions cease and the whole of the contents of the rumen turn sour. The rumen wall then becomes inflamed (rumenitis) making it more easy for toxins to be absorbed. It is the effect of these toxins, producing liver damage, a generalised metabolic acidosis, and then shock which can eventually lead to the death of the animal. Plate 13.10 shows a red and inflamed rumen wall from a cow which died from overeating fresh sugarbeet roots. Even if such animals survive, the rumen wall may be permanently scarred (Figure 3.1), leading to poor absorption of nutrients, or infection may ‘leak’ through the rumen wall to produce liver abscesses and subsequent depressed performance. Liver abscesses can be quite a problem in barley beef or feedlot cattle.
The detailed rumen changes associated with acidosis are described in Chapter 6. The normal rumen pH is 6.0-6.5, whereas with acidosis it may fall to 4.5-5.0. At pH 4.0 death is almost certain. As the pH falls, the cellulose-digesting protozoa especially start to die, which further depresses feed (forage) intake.

Plate 13.10. Rumen acidosis due to overeating. This cow died from eating an excess of sugarbeet. The rumen wall is very red and inflamed (rumenitis) and the normal black surface lining is peeled off far too easily.
Clinical signs
The clinical signs depend very much on the amount eaten and the time lapse since the animal gorged itself. If you are lucky, rumen contractions will continue and 18-24 hours after overeating the cow will develop a profuse, foul-smelling scour, containing whole particles of undigested grain. The beige-yellow colour, semi-solid consistency and foul smell of the faeces are almost diagnostic of overeating. There will be a drop in yield and the cow will be off her food for a few days, but apart from this there will be no other adverse effects.
If contractions cease and acidosis and toxaemia set in, then the syndrome is much more severe. The cow becomes very dull, her eyes sink and she may appear blind and start to stagger. In the early stages she may be almost constipated, although the faeces which are passed later will be typically foul-smelling and pale yellow in colour. When she becomes recumbent, stops drinking and grunts with every breath, the chances of recovery are very poor.
Treatment
Provided the rumen is still working, most cases can be treated medically. Sulphonamide by mouth (250 ml of a 33% solution) is very useful because not only does it stop the rapid bacterial fermentation, but being very caustic it also neutralises the acid in the rumen. One of the main groups of bacteria which proliferate are the lactobacilli, so penicillin can be used as an alternative to sulphonamides. Sodium bicarbonate (at least 250 g four times daily) can also be used as a neutralising agent, and large doses of water (10-15 litres or more three times daily), preferably given by stomach tube, help to reduce the concentration of lactic acid and thus prevent fluid from being withdrawn from the circulation. Calcium given intravenously or subcutaneously will stimulate ruminal contractions and both calcium and B vitamins assist the liver to metabolise the toxins absorbed from the rumen. Severely affected cows do in fact have a mild hypocalcaemia. Thiamine is a particularly important B vitamin to use, because there are often thiaminases present which destroy thiamine.
You must then watch your cow very carefully for the next 24 hours. If she deteriorates and no cudding or any other signs associated with ruminal movements can be detected, your vet will probably have to empty the rumen. This can be done surgically, by cutting a large hole in the left side (a rumenotomy) and removing the contents by hand. Alternatively, a large tight-fitting plastic tube can be passed into the rumen via the oesophagus, or through the skin, and the toxic products and concentrate ‘sludge’ washed out with water. This procedure is quite stressful to the animal, however, and she will need careful nursing afterwards. In beef cattle, casualty slaughter would be a better option.
Badly affected cows will have a metabolic acidosis as well as a ruminal acidosis and intravenous administration of calcium borogluconate and 300 ml of 5% sodium bicarbonate may help. However, care is needed because if an excess is given the cow develops alkalosis, which can be even worse. Oral administration of a 1:1 mix of magnesium hydroxide and magnesium carbonate helps to correct rumen pH. During the convalescent period supplement with B vitamins by injection, because as the rumen flora has been all but destroyed the cow could be short of B vitamins.
Cows which have overeaten high oil foods such as peanuts or precooked potato chips (waste products from the food industry) are much more difficult to treat. The oil coats both the bacteria and the food particles and seriously impedes rumen function. Casualty slaughter is then the best option.
The Cold Cow Syndrome
Following turnout to lush spring grazing, some cows develop a digestive upset which leads to a type of shock reaction. The symptoms vary considerably, but usually include dullness, off food, oedema of the vulva and a drop in milk production. Ruminal movements are poor, the dung has a partially digested appearance and it will probably be rather loose. The nose and skin of the animal feel cold and hence the name cold cow syndrome. Some cows are unsteady in their movements, almost as if they are drunk, and with a high pasture intake you are bound to suspect hypomagnesaemia. Most cows recover following symptomatic treatment, but it may be a while before milk yield returns to normal.
Various theories have been put forward regarding the possible cause and these include fungal toxins in the grass and the rapid fermentation of pasture with a very high sugar content. Personally I think that a contributory factor may also be a sudden intake of cold and very wet grass reducing the rate of fermentation by the ruminal bacteria. The rumen contents then turn sour, leading to stomach pain, the absorption of toxic products and scouring due to the passage of only partially digested food.
Rumen Impaction
In some ways impaction is similar to the cold cow syndrome. In this instance however the cow gorges itself on very dry or fibrous food, which becomes impacted as a hard, fibrous mass in the rumen. The symptoms are also similar, but generally much less severe. One dose of 500 g Epsom salts by mouth usually produces a cure, although on two occasions I have seen deaths from ruminal impaction, when very hungry animals had gained access to unlimited quantities of straw.
Wire (Traumatic Reticulitis)
This is one of the classic causes of stomach pain in the cow and it can also lead to other complications. Fragments of metal wire, copper flex, pig netting or even sharp bristles from a broom, which are accidentally taken in with the food, tend to drop into the reticulum. The recent increase in cases of ‘wire’ has been associated with the use of car tyres to hold down the plastic sheeting covering silage clamps. Over the years the tyres degenerate in the sun and small fragments of wire may fall onto the silage. Any tyres with crumbling rubber should therefore be discarded.
As the reticulum contracts the sharp-pointed object may penetrate its wall and with further contractions the object can slowly work its way into the peritoneal cavity, where the infection it has carried with it sets up a localised peritonitis. The position the wire normally penetrates is shown in Figure 13.3. Affected cows usually suffer a sharp drop in yield, they are off their food, dull, stand with their back slightly arched and they may be reluctant to move. They will have a raised temperature and will be slightly blown. The heifer in Plate 13.11 shows the typical stance of a wire. She has her head and one ear forward and her back is arched, depicting pain. Her tail is held up, but it is painful to pass dung. Her eyes are sunken. However, she is not bloated. The next stage in diagnosis is to listen carefully for the reticular grunt.
Earlier (on page 393) we saw that there were two phases of ruminal movements, so stand back and watch your cow from the left side. The left flank will move slightly as the first wave of contraction passes through the rumen and the cow belches immediately afterwards. This is activity in the upper ruminal sac. You then see another ruminal contraction, but without a belch, and at the same time the cow may grunt with pain. This second contraction is the mixing phase, and as the contraction passes through the lower ruminal sac and then the reticulum, the wire moves slightly, causing pain, and the cow grunts. This is an excellent diagnostic feature and is known as the Williams reflex.

Another test for a wire is to squeeze her back. As you pinch the skin she dips her spine. This stretches the reticulum and causes pain, which
Plate 13.11. Typical stance of a heifer with a wire. Her back is arched, tail slightly lifted because dunging is painful and her eyes sunken.
again elicits a grunt. The next time you squeeze her back she knows what will happen and will probably remain with her spine horizontal. The ‘pain grunt’ can also be evoked by lifting the reticular area, either by raising your knee underneath her stomach or by a pole held by two people, one each side of the cow.

Plate 13.12. Arumen magnet for treating a wire. The plastic case ensures that once attached, lengths of wire are not rubbed off by the friction of rumen movements.
lum (Figure 13.3) and a penetrating wire can easily cause a pericarditis (an infection of the pericardium, the heart sac, Plate 13.13). Whichever treatment is used, antibiotic therapy will be necessary to counteract peritonitis.
Vagus Indigestion
The vagus is the main nerve running to the rumen and it was once thought that vagus indigestion was a primary defect of this nerve. In fact the syndrome is an obstruction either of the outlet of the abomasum, when it is termed pyloric stenosis, or of the outlet from the reticulum, when it is called retic- ulo-omasal stenosis. The obstruction leads to a massive dilation of the rumen with fluid. The cow slowly goes off her food, over the course of days or even weeks. In the advanced stages she produces very little dung, her abdomen is grossly enlarged, similar to bloat, and she will be in a good deal of pain. If the obstruction is at the pylorus (pyloric stenosis), she will be even more sick, because of greater fluid imbalance changes. There is no treatment: casualty slaughter is the only available option. Most affected cows seem to have a low-grade inflamma-
Diagnosing a wire is certainly not an easy task and you are bound to want veterinary advice. The best treatment is to remove the wire by surgery. An alternative is a magnet (Plate 13.12) covered by a plastic case, approximately 10 cm long and 3 cm in diameter, which can be given by mouth and which pulls the wire back into the reticulum. If left untreated there is a risk that the cow may die, either from a more generalised peritonitis, or because the wire works forward to penetrate the heart. The heart is very close to the reticu- tion present, suggesting that the initial problem was possibly caused by a wire or some other form of localised peri-

Plate 13.13. This cow died because the wire (which can be seen in the picture) passed through the diaphragm and into the heart sac, producing a pericarditis. The outer sac (the
pericardium) and the heart itself are covered in pus.
tonitis.
Forestomach Obstruction
Cows which develop an obstruction of the forestomachs (rumen, reticulum or omasum) often display a characteristic ‘ten to four’ appearance. This expression is used because when viewed from behind (Plate 13.14), the cow appears swollen at the top of the left flank (‘ten to’) and at the bottom of the right flank (‘four o’clock’). Clinical signs are generally less acute and slower to develop than with intestinal torsion and it may be only after three to four days of low-grade illness that the rectum becomes empty. On rectal examination the rumen will feel grossly enlarged. There is no treatment and casualty slaughter is the best option.
Left-sided Displaced Abomasum
The abomasum is the fourth and last stomach of the ruminant. It resembles the true stomach in man, in that it is the site of digestion by enzymes produced by the stomach wall. It normally lies along the right side of the cow, just under the abdominal wall, as shown in Figure 13.4, and it is held in this position by attachments to the duodenum at one end and to the omasum at the other. However sometimes the abomasum passes underneath the rumen and up to the left flank, and lies between the skin and the upper sac of the rumen. This is a displaced abomasum. Gas accumulates and cannot

Plate 13.14. Forestomach obstruction, showing the typical ‘ten to four' appearance: abdominal enlargement at the top of the left flank and the bottom of the right flank.
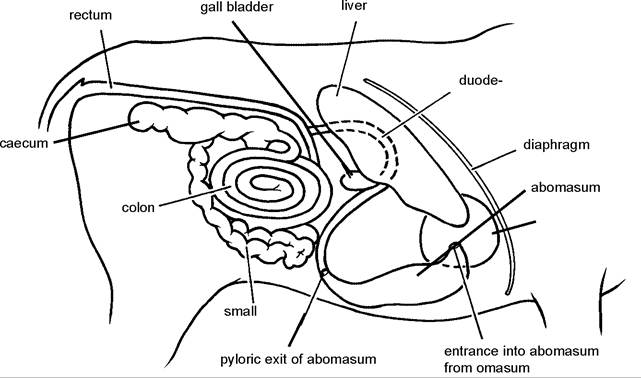
Figure 13.4. The normal position of the abomasum on the right flank.
escape because the duodenum is stretched under the rumen. If you listen carefully, you may be able to hear the gas and liquid making resonant splashing sounds under the left flank. It can be detected much more easily by flicking your finger onto the rib cage on the left side and listening for the resonance (described as a ‘ping’) with a stethoscope.
Disorders of the abomasum include
• left-sided displaced abomasum
• right-sided abomasal dilation and torsion
• abomasal ulcer
• abomasal bloat in calves (see Chapter 2)
Clinical signs
Probably the first thing you will see is a sudden drop in yield and the cow is off her food, especially her concentrates. In this respect the clinical signs are very similar to acetonaemia. After a few days a proportion of cows do in fact develop acetonaemia as a secondary symptom. Their dung tends to be very hard and they soon lose weight. The left flank over the rumen becomes distended due to the presence of the abomasum, and the cow may look slightly blown. It is not necessarily an acute condition, however, and some affected cows can live for several weeks. In mild cases the abomasum may even return to the correct position on its own, but the majority become displaced again a few days later. Acute cases occasionally occur, when the abomasum ulcerates or even ruptures and causes death, but this is rare.
Treatment
There are two main types of treatment and your vet will probably have his own preferences. By far the most successful is to open the cow surgically on her right flank and pull the abomasum back underneath the rumen into its correct position. It can then be sutured in place, thus preventing further displacement.
Surgery is expensive, however, and carries a degree of risk, so I like first to try to replace the abomasum by rolling the cow. If she is sedated and then laid on her back, the abomasum can be pushed from left to right over the top of the rumen by a pummelling action with the fists (Plate 13.15). It is almost always possible to replace the abomasum in this way, but unfortunately more than half the cases recur a few days later and still have to be treated surgically. Even so, I consider that this simple approach is worthwhile for the 30-40% of cows which do recover, and only a few days have been lost if the abomasum does displace again. After rolling, the cow should be put into the comfort of a straw yard and onto a high fibre:low concentrate diet, so that the rumen fills up and the abomasum is unable to displace underneath the rumen for a second time. Wait at least two weeks before bringing her back up to full rations.
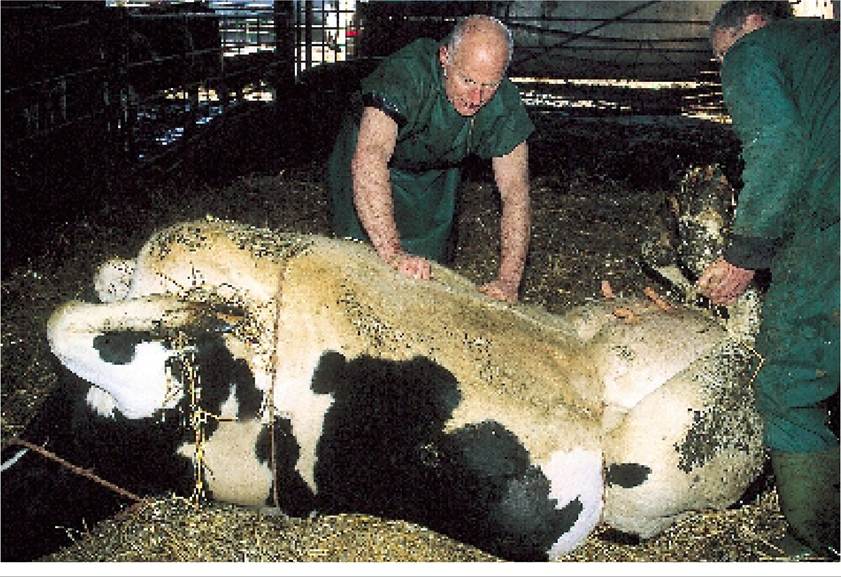
Plate 13.15. Correcting a displaced abomasum. If the cow is rolled onto her back, the abomasum can be pummelled across from left to right to return it to its original position.
Causes and prevention
The abomasum is suspended by attachments to the duodenum at one end and the omasum at the other (see Figure 13.4), so that as it contracts during normal digestion it pulls itself into the correct position. Displacement occurs when these abomasal contractions are weak or absent, or sometimes when a bubble of free gas accumulates. A displaced abomasum is most commonly seen in high-yielding cows in early to peak lactation. Potential causes include:
• high concentrate diets
• low fibre diets and especially diets with inadequate long fibre, both of which lead to poor rumination and acidosis. Adding hay, straw or big bale silage to the ration helps in prevention
• digestive upsets, which allow only partially digested food (especially starch) into the abomasum, where it may ferment to produce gas
• very high oil rations (those greater than 4.5% of the total diet), because excess oils suppress rumen fermentation
• a rumen that is not full, thus allowing the abomasum to pass underneath the rumen
• unsuitable precalving ration. All cows experience a reduction in appetite immediately before calving. An increase in nutrient density is needed to compensate; otherwise a degree of ketosis develops which can predispose to displaced abomasum.
• gross overfeeding, leading to overfat cows at calving and development of fatty liver (Chapter 6)
• an excessively rapid buildup of concentrates post calving can lead to acidosis (Chapter 6), which in turn predisposes to displaced abomasum
• stress. It has been shown that if some cows are simply taken out of the cubicles and put into the comfort and luxury of a straw yard, they will recover on their own
• intercurrent disease. A displaced abomasum often follows some other illness, for example recurrent milk fever, severe metritis, acidosis or fatty liver. It has been shown that cows with low blood calcium at calving are three to four times more likely to develop a displaced abomasum, even if they did not get clinical milk fever (see Table 6)
• sand accumulating in the abomasum (due to feeding dirty potatoes or fodder beet) may predispose, although one might expect this to hold the abomasum in position, rather than allowing it to displace
• there may be an hereditary predisposition - which could explain an increased incidence in some herds - associated with weak abomasal attachments
Right-sided Abomasal Dilation and Torsion
Sometimes the abomasum remains on the right side, but either twists over on itself (torsion) or simply undergoes gross dilation. Instead of lying in its normal position on the floor of the abdomen, the dilated organ may occupy the whole area under the ribs on the right side, from belly to spine. A resonant ‘ping’ can be heard when the ribs are tapped with the fingers, sounding identical to left displacement (but obviously on the right-hand side). Cows with right-sided dilation and/or torsion tend to be more seriously ill than those with left displacement. Mild cases may be treated medically for a few days, using drugs such as metoclopramide, which contract the abomasum. More severe cases need to be surgically opened and drained. Most animals recover quite well. There has been an increase in incidence in the UK, perhaps associated with the increased feeding of maize silage.
Abomasal Ulcer
Stomach ulcers are, of course, common in man and they also occur periodically in dairy cows. Many of the cases which I have seen have been in early spring or in the autumn, when the cows are grazing lush grass with a high nitrogen content. The initial symptoms are mild abdominal pain, a drop in yield and loss of appetite. There may or may not be a slight increase in temperature. Many ulcers bleed profusely, and when the blood is passed the dung turns to a dark, black, tar-like scour as in Plate 13.16. Badly affected cows will need a blood transfusion and some animals die, either from excessive blood loss or perforation of the ulcer leading to peritonitis. Blood transfusions may be difficult to justify economically. There is nothing to say that the ulcer has stopped bleeding, and giving blood will increase blood pressure and may even start further bleeding.
Less severe cases can be treated medically using kaolin and astringents (e.g. 20 g copper sulphate) given by mouth to try to arrest the bleeding, and iron injections to assist with re-forming blood. Dosing the cow with 60-100 ml of 10% sodium bicarbonate first may help to close the oesophageal groove (Chapter 2) and may allow the kaolin and copper sulphate to bypass the rumen and go
straight to the abomasum.
High yields, high concentrate diets and stress have all been suggested as potential causes. Low-grade abomasal ulcers are common in young calves.
Intestinal Obstruction (Stoppage)
A blocked intestine can arise from a range of different causes, three of which are described in the following.
Intestinal torsion (twisted gut) The intestine is suspended from the animal’s spine by the mesentery, and resembles a small piece of tubing running around the outside of a fan (Figure 13.4). Sometimes the whole mesentery twists over on itself (a twisted gut) or

Plate 13.16. Abomasal ulcer. The loose, black, tarry faeces seen around the tail of this cow are typical of an abomasal ulcer.
Disorders of the intestines include
• Obstruction (stoppage) from
- intestinal torsion (twisted gut)
- intussusception
- gut tie
• winter dysentery
• dilation and torsion of the caecum
• Johne's disease
• infectious and management causes (see Chapter 2)
perhaps only one segment of the intestine is twisted. This cuts off the blood supply to the intestine and causes a blockage (Plate 13.17).
Intussusception A length of intestine may telescope into an adjacent piece, as shown in Figure 13.5. This constricts the blood supply and leads to a swelling which in turn obstructs the flow of food material. The intestine below the obstruction will be empty but otherwise normal. The length above will be distended with accumulating intestinal contents. Very occasionally the constricted intestine sloughs off and is discharged in the faeces and the two opposing edges of the intestine heal naturally (A joins to B and C joins to D in Figure 13.5). However, this is rare.

Plate 13.17. Intestinal torsion (twisted gut). The post-mortem knife marks the point of the torsion. The dark-red dilated loops of intestine on the left are degenerating and have a very different appearance to the normal cream-coloured intestine on the right.
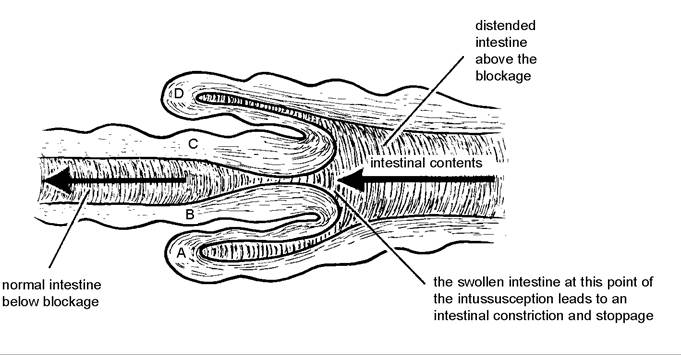
Figure 13.5. An intussusception: a segment of intestine telescopes into the piece behind. This constricts the blood flow and leads to a stoppage.
Gut tie (pelvic hernia) This can only occur in male calves which have been surgically castrated. A length of intestine prolapses through a small tear in the sheet of mesentery which originally carried the vas deferens. It then twists and becomes obstructed. This may occur several months after the castration, by which time the calf may be large enough for a rectal examination to be performed. The hole in the mesentery can then be enlarged manually, the loop of intestine is freed and the calf recovers rapidly. In other cases surgery may be needed.
Clinical signs
The clinical signs of a stoppage are similar, whatever the cause, although they will vary depending on the severity (partial or complete) and the position of the obstruction (whether near to the abomasum or near to the rectum). Initially the animal is dull. It picks at its food or stops eating altogether. It may show signs of colic, by kicking its flanks, looking at its sides or perhaps getting up and lying down repeatedly, in obvious discomfort. Some dry dung may be passed in the early stages, possibly covered with mucus, but later the rectum becomes sticky and empty. The animal’s temperature will probably be below normal and its pulse very fast.
If left, most animals will develop peritonitis and die. In valuable animals an intussusception can be treated surgically by resecting the obstruction, and gut tie may be released by surgery or by rectal manipulation, as described above. However, for most cases prompt casualty slaughter is the best option.
A word of caution: cows and young stock can develop colic simply from a spasm in the gut, that is from excessive muscle contractions. This will give symptoms very similar to the initial stages of a stoppage, but it is a colic which responds rapidly to treatment with muscle relaxants, so make sure that you get your vet to examine the animal before sending her off. This temporary colic syndrome is particularly common in young stock.
Winter Dysentery
Waves of scouring may pass through dairy herds, especially during the winter housing period, when the risk of faecal contamination is much greater. Some authorities consider that BVD is the primary agent of this so-called ‘winter dysentery’ of dairy cows, although others consider that a coronavirus infection is involved. In the first year that disease is seen, up to 80% of cows may be affected by this condition over a two to three month period, each animal running a temperature for a few days, scouring, off its food and with a sharp drop in milk production. Mouth and nose lesions are very rare. Occasional cases develop a very severe scour and die within a few days. However, the majority recover, although yield may be affected for the remainder of the lactation. During the second winter, further cases may be seen, but far fewer in number, and thereafter the disease becomes endemic in the herd, producing only occasional cases each winter, especially in heifers or purchased cows. Although winter scour is not too serious, it does cause a considerable nuisance and loss of milk.
Dilation and Torsion of the Caecum
The caecum is a blind-ended sac which is part of the large bowel (Figure 13.4). It lies under the right flank high up towards the spine, and torsion and dilation can occur in the same way as with the abomasum. The symptoms are very variable: mild cases present as a low-grade digestive upset and can be treated medically or simply left to recover on their own. More severe cases often produce marked abdominal pain and need to be surgically drained and deflated.
Johne’s Disease
Johne’s disease is an infection caused by Mycobacterium johnei. The bacterium is related to tuberculosis and this is why Johne’s is sometimes called paratuberculosis. Infection is taken in by mouth and produces a thickening of the lower part of the small intestine and the upper large intestine, although lesions can sometimes extend down as far as the rectum. The thickening interferes with the function of the gut, particularly the absorption of water and nutrients. Disease is usually seen following the stress of calving. The cow develops a profuse watery diarrhoea which characteristically froths when it hits the ground. Symptomatic treatment with kaolin, chlorodyne or astringents such as sulphonamides or copper sulphate may temporarily alleviate the scour, but it soon returns.
The other prominent feature of Johne’s disease is a massive weight loss. This continues until the cow is so thin and emaciated that she cannot stand and she dies from an inability to absorb the nutrients from her food. No animals should ever be allowed to reach this stage, of course, and once the diagnosis has been confirmed with a blood or dung sample, casualty slaughter is indicated. Johne’s disease provides a good example of bacteria which live inside cells and are therefore protected from the action of antibiotics. Tuberculosis and brucellosis are similar.
Although typical Johne’s disease is by no means as severe a problem as it used to be in the UK, the move towards larger herds has produced an increased incidence. There is evidence that it can persist in a subclinical form for eight to ten years or more, and may be a cause of chronic poor growth and disappointing production. These cows will be intermittent excretors of infection and will perpetuate the disease within a herd. They may transmit infection to their calves, both across the placenta and via colostrum. In one study around 30% of all calves born to clinically affected cows were positive to Johne’s, and even 10% of calves born to subclinically affected cows were positive. All calves from Johne’s cows should therefore be considered as suspect carriers. There is an additional danger in using pooled colostrum in an infected herd, because this could also be spreading infection.
Control of Johne S
Calves up to six months of age are the only animals in which infection can become established, but because the incubation period is two years or more, disease will not be seen until after the first or second calving at least. The stress of calving often precipitates the onset of scouring and at this stage the dung will contain massive numbers of Johne’s bacteria. Important control measures are therefore to remove the calf from its mother immediately after birth, to isolate affected animals and thus to avoid further faecal contamination of the environment, to identify and cull infected animals as soon as possible, and to make sure that feed and drinking water have not been infected. Unfortunately there is no good test to positively identify carrier animals. Probably the two major reasons why Johne’s is now less common are that calves are removed from their dams soon after birth and that clean water troughs have replaced drinking from dirty farm ponds.
In herds where Johne’s is a problem, vaccination can be carried out. A special licence may be needed, because the vaccine can interfere with the interpretation of the tuberculosis test. Calves are vaccinated during the first four weeks of life, by means of a subcutaneous injection into the dewlap between the front legs. Check that a hard nodule has formed. This indicates that there has been a good vaccine ‘take’. As two to three weeks are required for the vaccine to become effective and as it will not protect against a very heavy challenge of infection, vaccination should always be combined with the hygiene and management measures described above.
Relationship to Crohn S Disease in man
Johne’s bacteria have also been isolated from a few cases of people suffering from a human intestinal malabsorption syndrome known as Crohn’s disease. Although the link is by no means certain, the finding that pasteurisation did not fully remove all Johne’s bacteria from milk, and that up to 5% of samples of milk tested were positive for Johne’s, caused some concern in the UK. Pasteurisation times have now been increased, so the risk will be negligible. Even so, it is important to test all cases of chronic diarrhoea in adult cows, thereby removing any risk to both animals and man.
Liver Fluke (Fascioliasis)
The liver plays a vital part in dealing with the products of digestion and so I have included liver fluke in this section. Fluke is caused by a small parasite called Fasciola hepatica and hence sometimes the disease is called fascioliasis. It is an important condition in both sheep and cattle and is especially common in areas that are warm and wet.
Life cycle
The life cycle of the fluke is shown in Figure 13.6. Taking the adult egg-laying fluke in the liver as our starting point, fluke eggs may be shed in the dung throughout the winter, but it is only when the weather becomes warm (above 10°C) and wet that they begin to hatch. Hatching releases the miracidia and these swim around in a film of moisture until they contact and penetrate the snail Lymnaea truncatula. There is
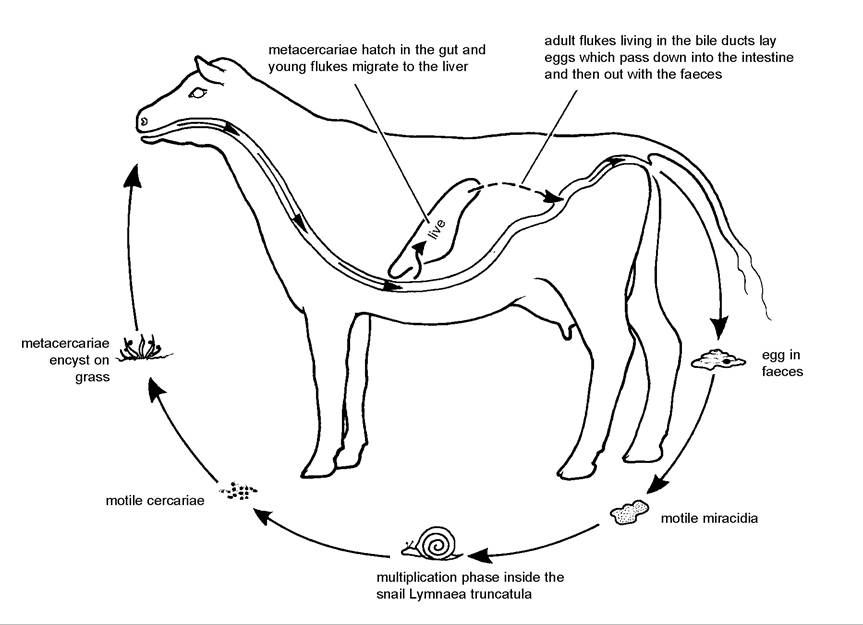
Figure 13.6. The life cycle of the liver fluke, Fasciola hepatica.
a multiplication phase inside the snail, so that one fluke miracidium entering the snail can lead to the release of over a thousand fluke cercariae from the snail. Cercariae swim onto blades of grass and encyst to form resistant structures, the metacercariae. After infected pasture has been eaten by cattle, the metacercariae hatch in the intestine to produce immature flukes. These migrate to and then burrow across the liver, continually feeding as they pass through its substance, until they reach the bile ducts. In the bile ducts they complete their final stage of development to adult egg-laying flukes. The eggs pass down to the gall-bladder, into the intestine and then out in the faeces, thus starting another cycle.
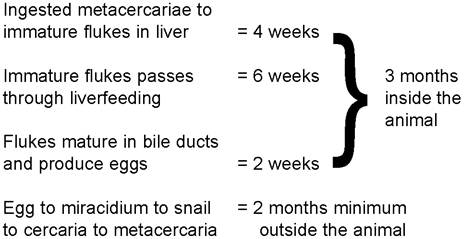
Compared with other parasites like husk or the stomach worm Ostertagia, liver fluke has a fairly long life cycle as shown in Table 13.2. The stage inside the cow, from eating the metacercariae until eggs are seen in the faeces, takes around three months, and even under favourable conditions, the stage outside the animal, that is the hatching of the eggs, development through the snail and production of metacercariae, takes at least another two months. By favourable conditions I mean a temperature above 10°C and plenty of wet weather. It is said that if there are eleven weeks of continuous wet weather, including the four weeks of June, this will produce ideal conditions for fluke. Hatching of the fluke eggs and the development of the snails are both stimulated by warmth and humidity, so if June and July are wet, all the fluke eggs which have been passed from December of the previous year onwards and which have overwintered on the pasture hatch at the same time as the snail population increases. This leads to a massive production of cercariae with a subsequent heavy infestation of metacercariae on the pasture. The metacercariae may be eaten by cattle from September onwards, but as adult flukes take three months to develop, there may be no significant disease seen until December or January. If, on the other hand, the summer months are either very dry or very cold, fewer fluke eggs hatch and there are fewer snails around anyway, so far fewer metacercariae encyst on the grass. This is the basis of the ‘Fluke Forecast’ issued by the Ministry of Agriculture in the UK. It is a very useful warning to farmers of when there is likely to be a high incidence of fluke and when treatments are necessary.
Table 13.2. Time spans in the fluke life cycle.
So far we have been talking about what is known as the ‘summer infection’ of snails. If September and October are warm and wet, then a second wave of fluke eggs may hatch and these weather conditions will also lead to an increase in the number of active available snails. By the time that the snail has become infected, however, the coldest weather will almost certainly have arrived and the snail then becomes dormant until the
Fluke populations survive the winter in three ways:
• as adult flukes in the livers of infected animals, which, if outwintered, will be continually passing fluke eggs which all hatch at approximately the same time to produce the summer infection of snails
• as resistant metacercariae on pasture
• as cercariae in dormant snails, the result of the winter infection
spring. As soon as spring weather conditions permit, snail activity starts again and metacercariae are deposited on the pasture. This is known as the ‘winter infection’ of snails. Clearly in the southern hemisphere winter and summer apply but the months will be different.
Summer infection of the snails is by far the most common, producing pasture infestation with metacercariae in the autumn, so that disease can be seen from December onwards, but usually not until January and February. However, as metacercariae can persist on grass over the winter and as snails can carry cercariae until the following year, it is possible to get outbreaks of fluke in the spring or even in the

Plate 13.18. Liver fluke. The bile ducts are grossly thickened, giving a classic ‘pipe-stem' appearance. Adult flukes can sometimes be squeezed out of the bile ducts. They are easily
summer. visible to the naked eye.
Cattle slowly build up an immunity to fluke and they seal them off in their bile ducts by laying down a thick, fibrous barrier, reinforced with calcium. This produces the classic ‘pipe-stem’ liver seen on post-mortem (Plate 13.18). The immunity limits the life span of the adult flukes to approximately one and a half years, so continual reinfestation of dairy cows is needed to maintain fluke populations.
Clinical signs
Although immature flukes cause some damage during their migration, the main effect is due to the bloodsucking activities of the adult flukes in the bile ducts. There is no ‘acute fluke’ type of disease as is seen in sheep. The blood loss leads to anaemia, and affected cattle look in poor condition, with rough staring coats, and they are generally unthrifty. Occasionally they develop a ‘bottle jaw’ appearance, due to the accumulation of fluid (known as dropsy or oedema fluid) under the skin of the chin, although again this symptom is much more commonly seen in sheep. In dairy cows quite low fluke burdens will depress protein in milk, and heavier infestations can lead to reduced yields. I have seen beef suckler cows so badly infected that many went down after calving and never recovered. Scouring is not a common feature of fluke and outbreaks of scouring in animals in poor condition in February or March are more likely to be due to type II Ostertagia (see Chapter 4). Liver fluke may increase the susceptibility of cows to Salmonella dublin infection.
Treatment and control
Only the drug oxyclozanide is currently licensed for use in milking cows in the UK, and there is a milk withholding period. On fluke farms the dairy herd should ideally be drenched twice during the winter period; for example, once in late December and then again in early February. The second dosing needs to be at least two and a half months after housing, so that all the metacercariae which were eaten during the autumn have reached adult stage and are then susceptible to the drug. If there is only a low risk of infestation, the first dose can be omitted. Outwintered cows and heifers which could have been eating infected pasture throughout the winter ought to receive a further dose in March or April.
Some drugs such as nitroxynil, rafoxanide and triclabendazole kill flukes at a much earlier stage of their life cycle and are very good to use in young stock and non-lactating animals. A single dose four weeks after housing should be adequate in the majority of cases.
The other aspect of the control of liver fluke is either to remove the snail habitats by drainage, or simply to fence them off. Cattle can then neither graze in these areas and become infected, nor dung there to deposit fluke eggs to infect snails with miracidia. Lymnaea truncatula snails prefer to live in a moist environment. They like the puddles beside streams and ponds or even hoof-marks in the mud if the ground is very wet. They do not like very acid soils such as peat bogs, so the application of lime to increase soil pH may lead to an outbreak of liver fluke. Under adverse conditions such as the cold in winter, or a very dry summer, snails become dormant and do not allow flukes to multiply.