The Situation in Africa
Before the detection of the presence of the indigenous Af1 and Af2 strains of M. bovis that, respectively, existed in Western and Eastern Africa before colonization, it was for long assumed that BTB was introduced by the settlers into the various African countries during the time of colonialism, particularly in the eighteenth and nineteenth centuries, by importing European cattle suffering from BTB (Michel 2008).
During that time, it became a well-known livestock disease in many parts of Africa (Manley 1929).The first recorded case of BTB in Africa was diagnosed in cattle in South Africa in 1880 (Hutcheon 1880), and it was subsequently diagnosed in 1888 in camels in Egypt (Mason 1912). Although there were differences of opinion, it was generally assumed that BTB was rare in indigenous livestock. Du Toit (1936) claimed that “judging by the reports of the veterinary authorities in Kenya, Anglo-Egyptian Sudan, the Gold Coast and Tanganyika,” BTB is relatively unimportant in tropical Africa. As support for this opinion, only 18 cases of BTB were recorded in Sudan from 1933 to 1950 (Awad 1962). Carmichael (1938) though stated that “TB is not by any means a new disease to the tropics, and that neither man nor his domestic animals constitute that “virgin soil” in which the tubercle bacillus can seed itself.” The general approach that BTB was not important was enhanced by the false assumption, based on anecdotal information, that the indigenous African zebu cattle were more resistant to contracting BTB compared to European cattle in which the infection progresses very rapidly. Known exceptions at the time were the straight- backed Ankole cattle in Uganda where during the early 1900s, more than 10% were found to be tuberculous (Carmichael 1938). However, as in Madagascar, and in India where a prevalence of BTB of up to 15% was recorded in zebu cattle during that time (Du Toit 1936), African zebus also proved not to be resistant to contracting the disease.
This misconception about the zebu’s perceived resistance to BTB contributed to the prevailing complacent attitude about the problem and the lack of its control in Africa (Awad 1962).Through the course of time, BTB was detected in more and more African countries. The disease was diagnosed in the British Cameroon in 1929 following the importation from Germany of purebred stock cattle owned by a German company (Manley 1929). In a similar vein, BTB in cattle became widespread in the 1930s in Morocco soon after the importation of European cattle breeds by the French settlers (Berrada (1993). The same pattern was recorded in French West Africa, the British Cameroon, and Northern Rhodesia (now Zambia) where large numbers of cattle were affected (Du Toit 1936). From 1925 onward, BTB was recorded in cattle in an increasing number of African countries, such as in Cameroon, Mali, Senegal, Nigeria, Somalia, Sudan, Tanzania, Uganda, Zimbabwe (Carmichael 1939), Egypt, Uganda, and Sudan (Awad 1962) and in camels (Elmossalami et al. 1971) and cattle in Chad (Diguimbaye-Djaibe et al. 2006).
BTB became widely disseminated throughout Africa as this generally chronic disease, when left uncontrolled, spreads throughout a herd and between herds following the uncontrolled movement of cattle from infected to non-infected herds, often across international boundaries (Francis 1959). From the available data, it appears that its prevalence increased considerably on the continent over the years, primarily because of the lack of any form of control and the primitive methods of animal husbandry that were practiced in large parts of the continent (Carmichael 1939).
Not only did the disease spread throughout the continent, but its prevalence also increased, although in a patchy fashion. An example is the situation in Nigeria, where 42% of carcasses condemned between 1975 and 1977 were due to BTB (Opara 2005). Also in Nigeria in 1981 and 1990, 0.09% and 4.2% of carcasses examined, respectively, were fully or partially condemned due to BTB (Alaku and Moruppa 1993).
Particularly high prevalences were detected in the Western Province of Zambia, where from 2000 to 2003, BTB was responsible for 83.1% (n = 183) of carcass condemnations (Munyeme et al. 2010). Losses because of the disease became extensive, and over 32 tons of beef and beef offal were condemned due to BTB in Togo from 1985 to 1987 (Domingo 2000) and this in countries that could ill afford the loss of protein of this dimension. Not dealing with the problem of BTB and the absence of animal identification to trace infection back to its source led to further dissemination of the disease and an increase in numbers of infected cattle. The mere counting of infected tissues, year after year, did not, and will not aid the control of the infection, and will not reduce the prevalence of BTB (Amanfu 2006).In spite of the high prevalence in certain countries, such as Cote d’Ivoire, where nearly 50% of whole and 46% of partial bovine carcasses condemned in 1992 were attributed to BTB, the authorities appear not to be concerned as during that time, only one outbreak of BTB was officially reported (Benkirane 1998). This type of practice implies that because data on zoonotic diseases are collected in a passive manner and from a wide range of sources, including abattoir records (Table 2.1), they are unlikely to reflect the actual situation, and it is likely to result in a substantial underestimation of the magnitude of the problem. In addition, available data are not fully analyzed, and in most of the countries, little is done in terms of mitigation following the detection of tuberculous cattle.
Table 2.1 Status of bovine tuberculosis in 54 African countries (2016) (OIE 2017)
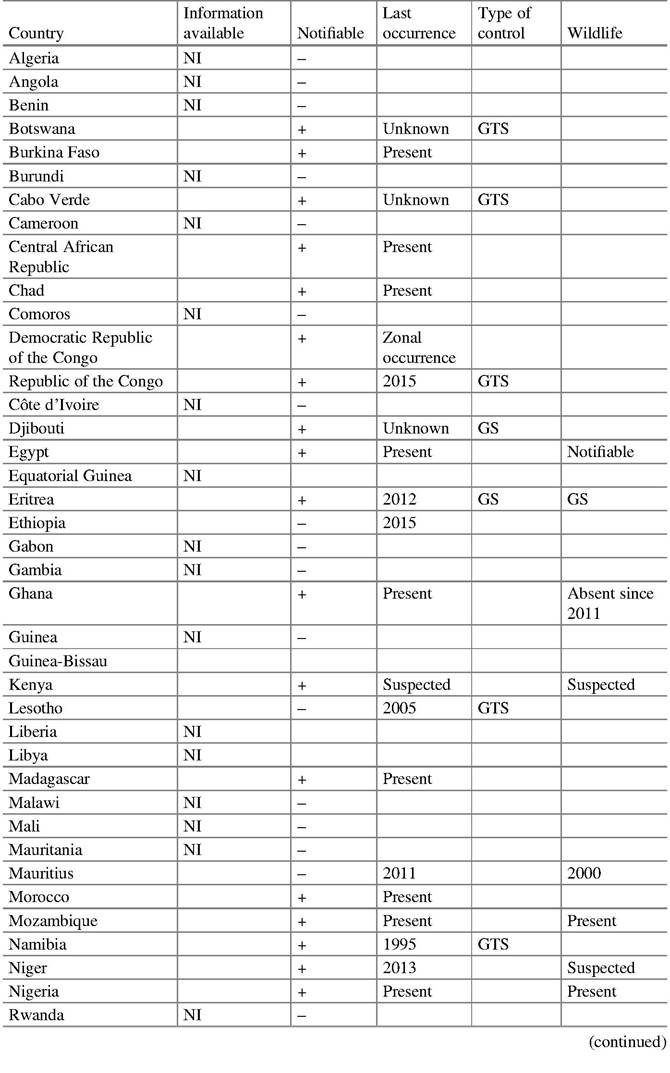
Table 2.1 (continued)
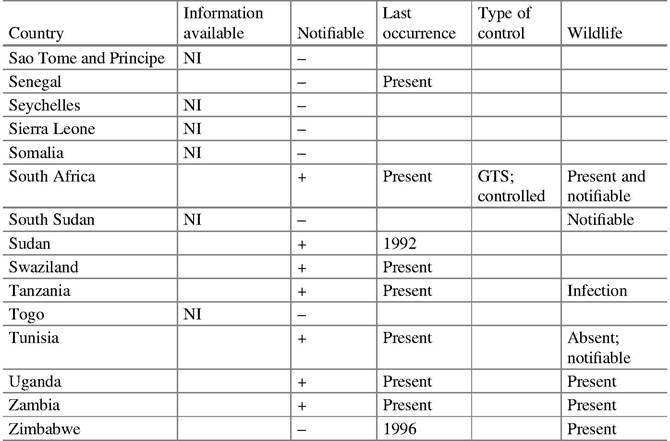
NI, no information provided either over time for all diseases or specifically for BTB; +, notifiable disease; -, not notifiable; GS, general surveillance; GTS, general and targeted surveillance
The complacent attitude toward BTB is enhanced by the assumption that in extensive farming practices, close contact between animals is limited, and the spread of M.
bovis in these herds is expected to be slow, and the prevalence low. Under such circumstances, it is argued that BTB will remain at low endemic levels, and there is thus scant motivation for regulatory authorities to apply the complex and expensive internationally accepted control measures required for its control and eradication (Benkirane 1998). In addition, the general apathy and lack of knowledge of African herdsmen about the importance of diseases that do not cause immediate losses complicate the processes of detection and reporting the occurrence of BTB in Africa (Carmichael 1939). This attitude still prevails, and in a Participatory Rural Appraisal (PRA) conducted in the Gambia, Senegal, Guinea-Bissau, and Guinea, for instance, participants ranked hemorrhagic septicemia and “diarrhea complex” (in cattle) and Peste des Petits Ruminants (PPR) (in small ruminants) high in the “general disease” survey. From the list of zoonotic diseases, only brucellosis (hygroma) made it to the “top 10” list in one country. Of the four zoonoses (rabies, anthrax, BTB, and brucellosis) incorporated in the analysis, only rabies was ranked high. Bovine TB was not known by any of the study subjects (Unger and Munstermann 2004). This is likely to be the situation in many, if not most, African countries.Through the years, veterinary authorities in Africa were concerned with the more economically important, rapidly fatal, and usually transboundary animal diseases such as rinderpest, contagious bovine pleuropneumonia (CBPP), East Coast fever, and anthrax, which from time immemorial ravaged the herds in tropical countries (Carmichael 1939; Alaku and Moruppa 1993). There was consensus that compared to the effect of the major endemic diseases prevalent in the developing countries, the overall economic impact of BTB on livestock production in Africa was assumed not to be important, and in most countries, this prompted regulatory authorities not to implement the costly control strategy at national and regional levels (Berrada 1993).
The insidious nature of BTB enhanced the justification of this approach, but there seems little doubt that the disease has been quietly progressing for many years both in humans and animals (Carmichael 1938). Currently, the disease is present in many African countries, but due to the lack of financial and human resources, and the political will, only a few of them conduct any form of surveillance or attempt to apply adequate control measures. As a consequence, the extent and the epidemiology of BTB in Africa are largely unknown, and the disease, with few exceptions, is mostly diagnosed during meat inspection in abattoirs, which itself is a very rough measure of the extent of the infection, and by the very limited use of routine tuberculin skin testing.According to the OIE’s WAHID (OIE 2017), 24 of the member countries have not provided any information about the presence of BTB during the course of time, and it remains unknown whether the infection is present in these countries (Table 2.1). Of the countries that include cases or outbreaks of BTB in their reports to the OIE, only 28 consider it as important enough to deal with as a notifiable disease in livestock, and only four list it as a notifiable disease in wildlife.
2.4