ASSOCIATIONS BETWEEN PROTEASE MUTATIONS AND CLINICAL OR CD4 OUTCOME
The impact of protease mutations was studied extensively from the viral standpoint, but the effect of protease mutations upon the clinical course of disease received less attention.
An emerging literature suggests that mutations in PR may be associated with a slower course of disease progression. Much of this literature is embedded in the literature concerning discordant response to therapy, in which the majority (if not all) of patients with immunologic discordance have viral isolates with PR resistance mutations, impaired viral fitness, and, therefore, impaired protease enzyme catalytic activity.An association between infection with PI-resistant HIV and decreased CD4 cell loss could be envisioned to be the result of impaired catalytic activity of mutant protease (Figure 10.4). These protease mutations, which are selected for in the presence of PI, confer survival benefit in the presence of PI and possess decreased catalytic ability. The evidence linking HIV protease with mechanisms of cellular apoptosis suggests that mutant protease, with its decreased catalytic activity, also may have impaired ability to initiate apoptosis, thereby explaining an association between protease mutations and improved immunologic and clinical outcomes.
Because there is strong evidence that HIV PR induces cell death through apopotosis or necrosis, we hypothesize that PR inhibitor-resistant mutations might attenuate or enhance HIV protease ability to induce cell death. Indeed, some data suggest that PR mutation may slow disease progression.49 Recently, the hypothesis that impaired PR catalytic activity will lead to enhanced CD4 T cell counts was tested. In 191 HIV-infected patients, viral sequences corresponding to the terminal 18 amino acids of Gag, all of PR, and a proximal segment of RT were cloned from patient isolates. This sequence was inserted into an expression vector, and cleavage kinetics was compared with WT HIV (strain NL4-3).
Impaired fitness of PR was significantly associated with improved CD4 T cell counts by both cross-sectional and longitudinal analyses.69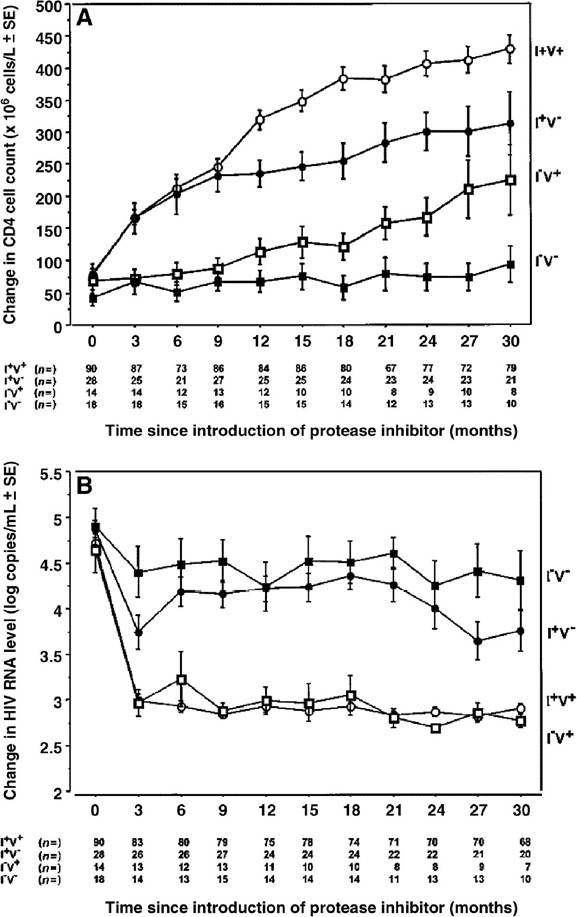
FIGURE 10.4 Changes in CD4 cell counts and plasma human immunodeficiency virus (HIV) RNA levels, according to immunologic and virologic status within the first 12 months of highly active antiretroviral treatment. (A) CD4 cell count changes ±SE. (B) Mean plasma HIV RNA level changes ±SE. Number of patients evaluated at each time point is shown. I+V+, patients with an immunologic and virologic response to therapy; I+V-, patients with a sustained increase in CD4 cells in the absence of a significant decrease in plasma HIV RNA or without a transient decrease in plasma HIV RNA; I-V+, patients with a decreased plasma HIV load without an increase in CD4 cell count; I-V-, patients without an immunologic or virologic response to therapy.
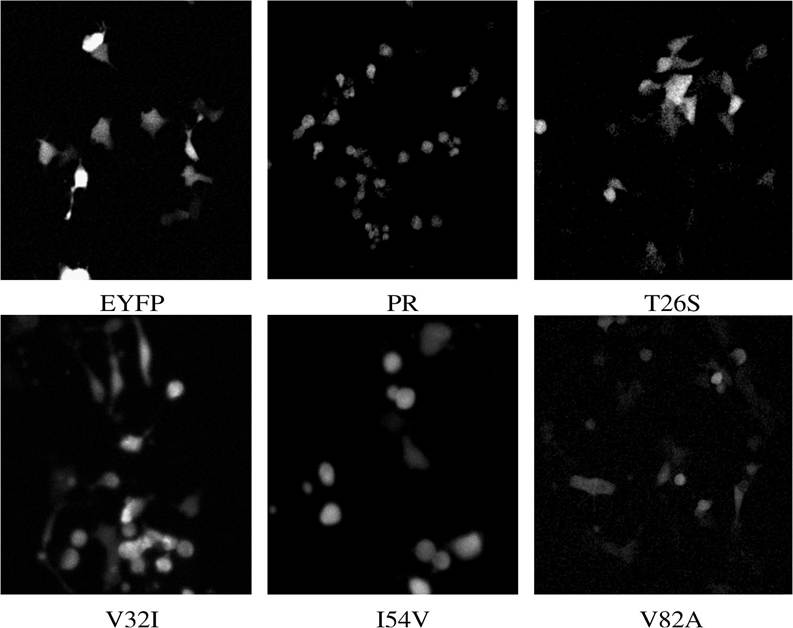
FIGURE 10.5 The cytotoxic effects of YFPPR and YFPPR primary mutants in transiently transfused 293 cells.