Clinical aspects of HIV disease in developing countries
As in industrialised countries, the spectrum of clinical manifestations associated with HIV infection is wide, ranging, as the CD4 count falls, from an asymptomatic state, through symptomatic disease, to fatal illness characterised by opportunistic infections, malignancies, neurological disease and wasting.
Initial acquisition of HIV infection (“acute HIV infection” or “seroconversion illness”) may be complicated by a syndrome resembling infectious mononucleosis, or a wide range of other manifestations as described in chapter 4. However, since this syndrome is not specific, it is rarely recognised even when clinically apparent.Early manifestations of HIV disease
Common early symptoms and signs are weight loss, fever, night sweats and diarrhoea. Skin disorders are frequent early manifestations, especially varicella zoster, fungal infections and pruriginous dermatitis, an itchy rash consisting initially of papules which become shallow ulcers due to scratching, and finally heal, leaving pigmented macules.
Tuberculosis
Tuberculosis is unquestionably the most important opportunistic infection complicating HIV infection in developing countries, and may present at any stage in the course of immunodeficiency. In early HIV disease, pulmonary tuberculosis is similar to that found in HIV-negative people. In advanced immunodeficiency, tuberculosis is often disseminated and multibacillary in nature. Nocardiosis, while much less common, is a differential diagnosis in some areas.
Bacterial septicaemia
An inadequately recognised manifestation of HIV disease in developing countries has been bacterial septicaemia. Gramnegative organisms are the most common pathogens identified, especially non-typhoid Salmonella spp. Invasive pneumococcal disease is also frequent, and may occur earlier than Gramnegative infections. In some patients with advanced HIV disease, mycobacteraemia is detectable; this is much more frequently due to Mycobacterium tuberculosis than Mycobacterium avium intracellulare complex.
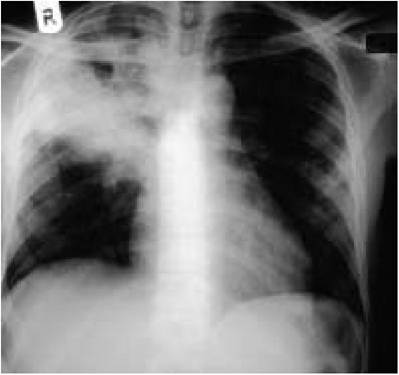
Figure 10.4 Chest radiograph showing upper lobe cavitation typical of pulmonary tuberculosis. Appearances may also be atypical (see chapter 6)
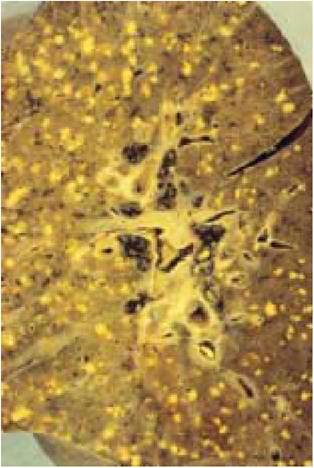
Figure 10.5 Post-mortem lung showing miliary tuberculosis (courtesy of Professor Sebastian Lucas)
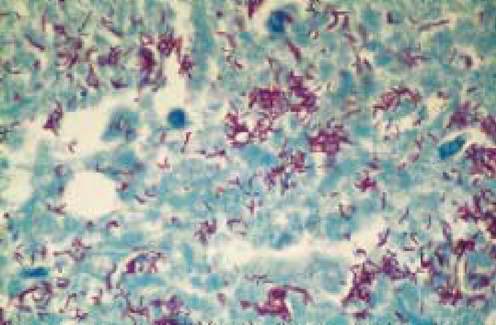
Figure 10.6 Tuberculosis may be multibacillary in HIV-infected patients: nonreactive tuberculous infection of the pericardium, showing abundant acid-fast bacilli (courtesy of Professor Sebastian Lucas)
Diarrhoeal disease and HIV wasting syndrome
The best known clinical picture of AIDS in Africa is “slim”, the term given by people in rural Uganda to the HIV wasting syndrome. Profound wasting, chronic diarrhoea and fever are the typical features. About half the time no specific aetiology can be found for the diarrhoea: among identified causes, the most common are cryptosporidiosis, microsporidiosis, isosporiasis and bacterial infections. The commonest autopsy finding in African patients with HIV wasting syndrome is disseminated tuberculosis, and undue emphasis may have been put on searching for a primary gastrointestinal cause of this whole syndrome. As with all medical causes of wasting, an important contributing factor to the HIV wasting syndrome is reduced food intake.
Neurological disease
Cerebral toxoplasmosis and cryptococcal meningitis are probably more frequent causes of severe HIV-related disease in developing than industrialised countries, and their prevalence may vary by geographical region. Cerebral toxoplasmosis most often presents as a space-occupying lesion of the brain, and cryptococcosis as a chronic meningitis.
Regional variation in disease spectrum
Tuberculosis and bacterial infections, particularly pneumococcal disease, are common HIV-related diseases in developing countries worldwide.
Other HIV-related diseases show regional variation. Pneumocystosis, cytomegalovirus disease and disease due to atypical mycobacteria such as Mycobacterium avium intracellulare, common in industrialised countries, are unusual in adults in many African countries (although Pneumocystis carinii pneumonia is common in HIV-infected African infants). The reasons for this are uncertain, but may include development of diseases such as tuberculosis at higher levels of CD4 counts, and shorter survival once the stage of profound immunodeficiency has been reached. Endemic Kaposi's sarcoma is more common in Central and East than in West Africa, and this is probably also true for the AIDS-associated form.Some HIV-related diseases are limited to specific geographic areas, such as disease due to the fungus Penicillium marneffei, which is confined to south-east Asia. Penicilliosis causes disseminated disease in patients with advanced immune deficiency, with nodular skin lesions as the most obvious manifestation. Tuberculosis, salmonellosis and cryptococcosis are other frequent AIDS-defining conditions in south and southeast Asia. Tuberculosis is frequent in Latin America, where the spectrum of disease is otherwise similar to that in the industrialised world.
Association with endemic tropical diseases
The association between endemic tropical diseases and HIV infection has only been studied to a limited degree. Theoretically, HIV infection could increase the incidence of tropical diseases, and alter their natural history, clinical expression, or response to treatment. Malaria is indirectly linked to HIV infection by causing anaemia in children, who may then be at risk for HIV infection transmitted through blood transfusion. HIV-infected pregnant women experience greater frequency and severity of malarial parasitaemia, and increased frequency of placental malaria compared with HIV negative women. HIV-infected people with Schistosoma mansoni excrete fewer eggs than those who are HIV negative, but it is not known whether the severity of schistosomiasis is affected by HIV infection, and response to treatment seems to be unaffected by HIV status.
Amoebiasis and strongyloidiasis might be expected to be more frequent in HIV disease, but are not; on the basis of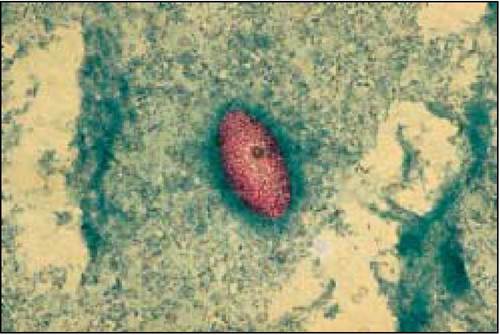
Figure 10.7 Isospora belli, a treatable course of diarrhoea in HIV-infected people
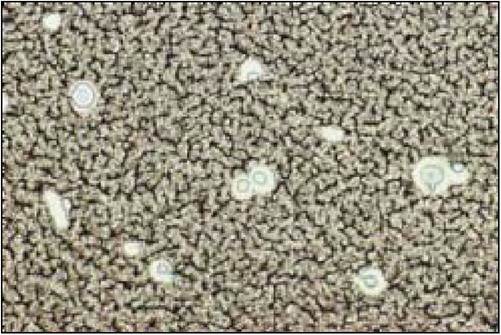
Figure 10.8 India ink stain of cerebrospinal fluid showing Cryptococcus neoformans, a common cause of meningitis (courtesy of Professor Sebastian Lucas)

Figure 10.9 Cerebral toxoplasmosis: haemorrhagic and necrotic mass in the occipital lobe (courtesy of Professor Sebastian Lucas)
limited data, the same seems to be true of trypanosomiasis and leprosy. Little information is available concerning the influence of HIV infection on filariasis. Visceral leishmaniasis, often disseminated, appears to be increased in incidence in HIV- infected persons, although most reports have been from southern Europe rather than sub-Saharan Africa or South America. HIV-infected persons with leishmaniasis require maintenance treatment as relapse is otherwise likely.