Clinical Presentation and Cardiovascular Risk Factors
The spectrum of CAD in HIV-infected patients is similar to non-HIV-infected patients with various clinical presentations including silent ischemia, stable angina, and acute coronary syndrome (unstable angina, non-ST elevation myocardial infarction, ST elevation myocardial infarction; Figs.
1-6). The first case of CAD in the HAART era was published in 1998 followed by several case reports and series [6-13].Whether protease inhibitors are directly responsible for CAD remains a matter of debate [5, 14].
In our cardiology department [13], 1 female and 19 male patients (mean age, 44±8 years; range, 34-65 years), infected with HIV since 9±4 years ago, were admitted from 1996 to 2002 for acute coronary syndrome (18 had myocardial infarction and 2 had unstable angina). Tobacco consumption (80%) and dyslipidemia (65%) were the most frequent cardiovascular risk factors. The median CD4 cell count was 387±184∕mm3 and the median viral load was 8,000±23,000 copies/ml. Fourteen patients were treated with protease inhibitors for a mean duration of 19±13 months. Five patients were treated with thrombolysis, three had primary angioplasty.
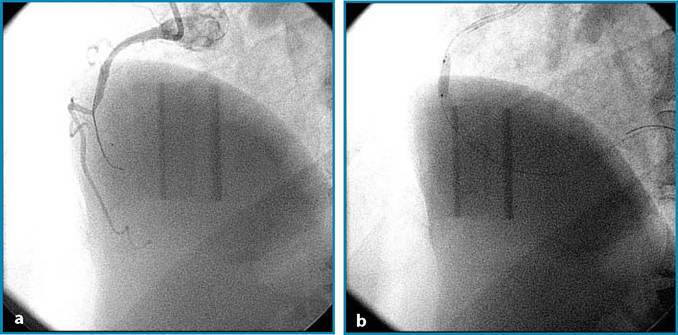
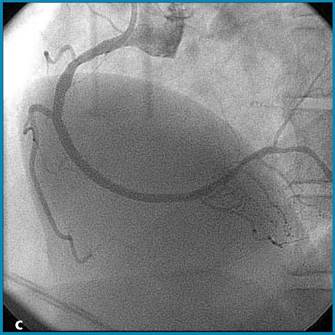
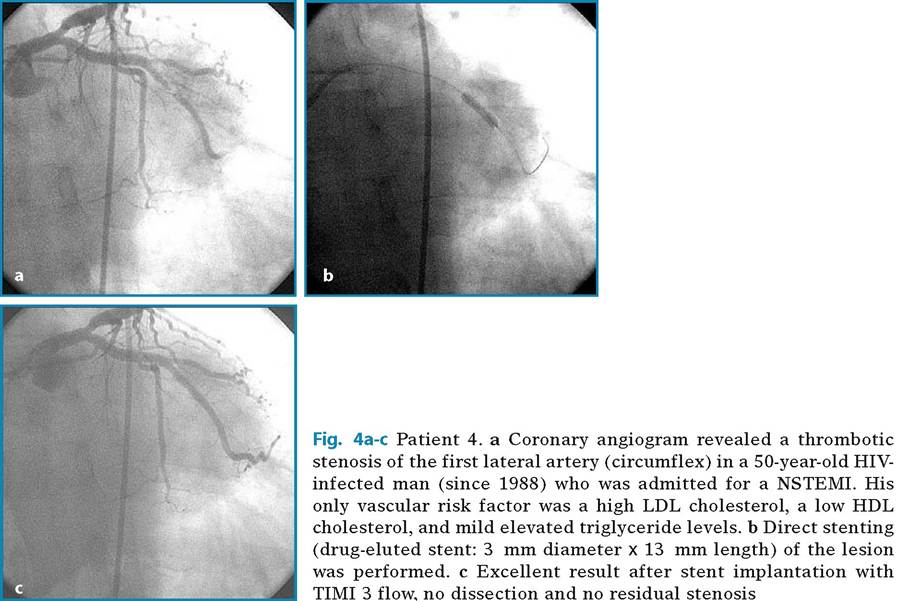
Fig. 1a-c Patient 1. a Coronary angiogram revealed an acute occlusion of the right coronary artery in a 38-year-old HIV- infected man (since 1995) during inferior acute myocardial infarction. A guide-wire is introduced into the lumen artery to pass the thrombotic occlusion. His vascular risk factors were smoking and mild dyslipidemia (high LDL cholesterol, low HDL cholesterol, and high triglyceride levels). b Balloon angioplasty performed at the site of the occlusion with 10- atmosphere expansion pressure. c Result after inflation of the balloon and implantation of a long bare stent (3.5 mm diameter, 32 mm length)
Fig.
2 Patient 2. Coronary angiogram finding a left main coronary stenosis (70%) in a 62-year-old HIV-infected woman (since 1987) who was admitted for an episode of unstable angina. Vascular risk factors were smoking and mixed dyslipidemia. She underwent a coronary artery by pass including the left internal mammary artery
Duong et al. [12] showed that silent myocardial ischemia (detected by treadmill test) was increased in HIV-infected patients without CHD (11%) and that age, central fat accumulation, and hypercholesterolemia were independent predictive factors. HIV- infected patients seem to be at higher risk of CAD than the general population as demonstrated by Bergersen et al. [15], who reported that compared to control subjects, twice as many HIV-infected patients on HAART had an estimated 10-year CHD Framingham risk above 20%. Neumann et al. [16], in a cohort of 309 HIV-infected patients, demonstrated that the risk of cardiovascular events is related to the age of HIV-infected patients. The overall 10-year probability for cardiovascular events was higher in the oldest group (>50 years; median, 20.5%) than in the youngest group (18-30 years; 1.9%; pSCORE). They observed that the Framingham equation categorized a higher proportion of HIV-infected male patients with moderate cardiovascular risk and a lower proportion of those with low risk (p6.2 mmol/L decreased from 21.1 to 12.3%. The prevalence of cardiovascular risk and CHD was higher in patients currently on antiretroviral (ART) therapy than in either pretreated or ART-naive patients.
In conclusion, HIV-infected patients undergoing HAART seem to be at a higher risk of CAD because of the higher incidence of traditional vascular risk factors [21-23] compared with same-age non-HIV-infected patients. Whether protease inhibitors have a direct impact on atherosclerosis remains hypothetical, however strong evidences now argue for a direct impact of protease inhibitors on the incidence of myocardial infarction [14, 24, 25].