Pathophysiology
Several hypotheses have been raised regarding the pathophysiology of atherosclerotic CAD in HIV-infected patients undergoing HAART. Many factors could increase the rate of cardiovascular events and accelerate atherosclerosis:
1.
Insulin resistance (reported in 25-62% of HIV-infected patients), diabetes mellitus (5-10%), and lipodystrophy syndrome (20-83%) [23, 26, 27]2. Resistant dyslipidemia-lower level of HDL cholesterol, higher level of triglycerides (50%-90%), small and dense LDL particles-with lower efficacy of lipid-lowering therapy [27-32]
3. Chronic inflammation and infection with increased cytokine levels (tumor necrosis factor-alpha, interleukin-1, interleukin-6, interleukin-10, monocyte chemoattractant protein-1) [33-37]
4. Enhanced endothelial injury due to dyslipidemia [38], oxidant stress [39], adhesion molecules [40], HIV Tat protein, related angiogenic effects [33, 41, 42] and immunological response [42]
5. A prothrombotic state linked to HIV status and/or antiretroviral therapy [43, 44] The role of metabolic disorders (low level of HDL cholesterol and hypertriglyceridemia) is highlighted in different studies [45, 46] that included HIV+ patients with acute coronary syndrome compared with HIV+ subjects without cardiovascular manifestations. These disorders can be partly explained by HIV treatments that result in higher hypertriglyceridemia and lower levels of HDL cholesterol compared with non- infected-HIV patients. The low level of HDL cholesterol may play a major role in the pathophysiologic mechanism of athero- thrombosis. Another aspect is the degree of the immunologic status reflected by the CD4 cell count level, which has been demonstrated to be lower in HIV+ patients with acute coronary syndrome compared with HIV+ patients without acute coronary syndrome [45, 46].
Direct vascular toxicity of the virus has been suggested in a report from Barbaro et al.
[47]. They found HIV-1 sequences within the arterial wall in a 32-year-old man without vascular risk factors who died from an anterior myocardial infarction. In addition, Schecter et al. [34] demonstrated that HIV- envelope glycoprotein gp120 activates human arterial smooth muscle cells to express tissue factor and promote the coagulation cascade and plaque rupture, supporting the observation of a correlation between plasma HIV load, a prothrombotic state, and cellular apoptosis.Tabib et al. [48] found that coronary artery lesions of young HIV-infected patients at autopsy, whose death was caused from other cardiovascular disease, were of an intermediate type, between those observed in coronary atherosclerosis and chronic rejection in cardiac transplant patients. Subclinical atherosclerosis in HIV-infected patients has been reported [42, 49-53] with increased intima-media thickness and atherosclerotic plaques of the carotid and femoral arteries correlated to age, dyslipidemia, and tobacco use, but not with protease inhibitor therapy. Coronary artery calcifications, another surrogate marker and prognostic factor of atherosclerosis visualized with electron beam computed tomography, are under evaluation in HIV-infected patients, with controversial results [54-56]. Coronary magnetic resonance angiography could be a further diagnostic tool for detecting infraclinic coronary atherosclerosis in the near future (Fig. 7).
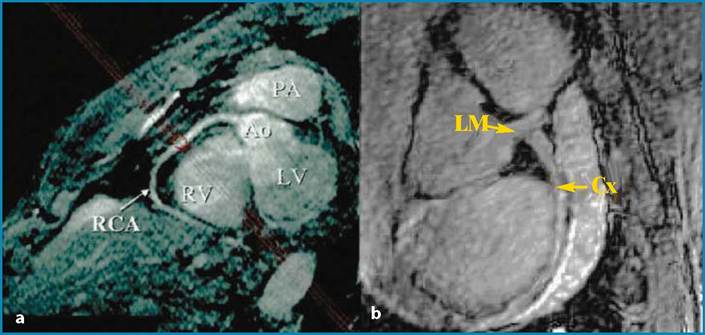
Fig. 7a,b Magnetic resonance angiography finding of normal coronary arteries. PA, pulmonary artery; Ao, aorta; LV, left ventricle; RV, right ventricle; RCA, right coronary artery; LM, left main coronary artery; Cx, circumflex