CMR of Myocardial Infarction
Coronary artery disease and ischemic heart disease are relatively common in patients with HIV infection [3, 4]. The prevalence of ischemic heart disease and its related mortality are increasing among HIV-positive patients [5,6].
The increased prevalence could be, at least in part, related to an improvement in the overall survival of HIV-positive patients, especially since the introduction of HAART. The origins of the disease appear to be multifactorial and related to the higher incidence of infection with herpesvirus, cytomegalovirus, or HIV-1, as well as to the inclusion of protease inhibitors, which have been reported to produce lipodystrophy, hyper- lipidaemia, and hyperglycaemia [6-8]. In a retrospective analysis of data from the Frankfurt HIV cohort, which included almost 5,000 patients, a fourfold increase in the annual incidence of myocardial infarction (MI) among HIV-infected patients was found after the establishment of HAART with protease inhibitors, compared with the incidence among patients who underwent treatment before the institution of HAART [6]. Histopathologic examination of coronary arteries generally reveals eccentric atheromatous and fibrous plaques, with variable degrees of chronic inflammation and accelerated atherosclerosis. Unusual proliferation of smooth muscle cells with abundant elastic fibers, as well as diffuse and circumferential involvement of the coronary arteries have been reported [1, 9, 10]. Investigators in the Data Collection on Adverse Events of AntiHIV Drugs Study, a prospective observational study of a cohort of 23,468 HIV-positive patients, found that the incidence of MI increased by an average of 26% per year of therapy with combined antiretroviral agents [11]. Not surprisingly, a further analysis of data from the same population indicated that these patients experienced an increased incidence and higher risk of other cardiac and cerebrovascular events (e.g. stroke; death from end-stage ischemic heart disease other than MI; and invasive cardiovascular procedures such as angioplasty, coronary bypass grafts, and carotid endarterectomy) [12]. Therefore, the diagnosis of cardiovascular disease by noninva- sive imaging is increasingly required in the HIV-infected population.Cine-CMR with steady-state free precession allows for accurate assessment of LV global and regional LV and RV function. Myocardial infarction appears as hypokinesia or akinesia during systole, which occurs in a myocardial wall supplied by an epicardial coronary artery (Fig. 1). Myocardial thinning may occur during systole. Besides rapid imaging of cardiac morphology, cine- CMR also permits the assessment of mitral valve regurgitation. Mechanical complications occurring after acute MI may be depicted by CMR in the cine mode. They include pericardial effusion, LV aneurysm, intracavitary thrombus, and mitral regurgitation (Fig. 2). Acute infarcts may be recognized as hyperintense signal on breathhold ECG-gated T2-weighted black-blood fast spin-echo CMR images during the first days after the onset of MI (Fig. 3) [13]. This technique, however, does not identify chronic infarcts and may overestimate infarct size by including area at risk. In addition, T2-weighted images often have a low signal-to-noise ratio. Dynamic ultrafast multislice CMR of myocardial perfusion allows for the detection of microvascular obstruction after MI (Fig. 4) [14], or may add significant diagnostic value over usual clinical and biological markers after non-
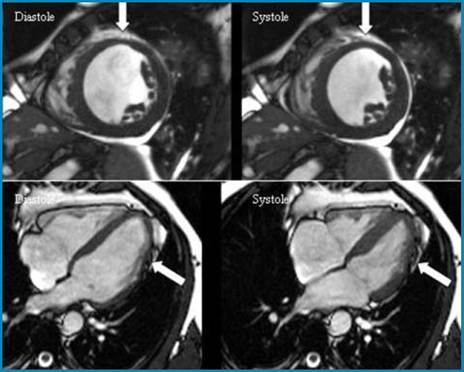
Fig. 1 HIV-infected 36-year old male with HAART who suffered a first recent anterior acute MI. Still images extracted from a cine- CMR sequence, performed at day 3, in the short axis (upper panel) and 4-chamber views (lower panel), at end-diastole (left) and end-systole (right), showing a segmental akinesia in the mid-anterior (upper panel, arrows) and apicolateral walls (lower panel, arrows), corresponding to the left anterior descending coronary territory
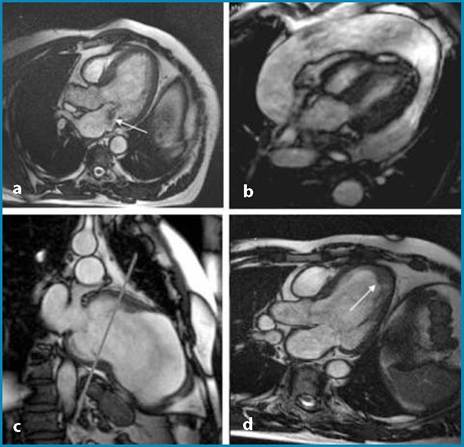
Fig.
2a-d Still frames extracted from cine-CMR in four different patients who presented with MI. a 3-chamber-view during systole, showing mitral regurgitation as a dark jet (arrow). b abundant pericardial effusion and cardiac tamponade. c Chronic MI, old apical aneurysm. d apical thrombus (arrow) complicating the course of anterior acute MI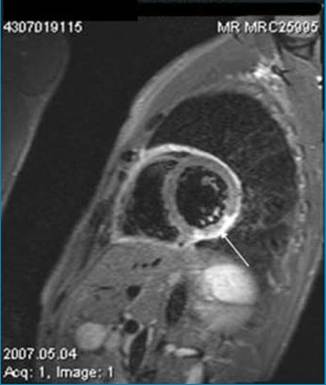
Fig. 3 42-year-old male with HIV and HAART. Pre-contrast T2- weighted black-blood fast spin-echo CMR image in the shortaxis view showing a hypersignal in the inferolateral wall (arrow) 2 days after the onset of acute MI
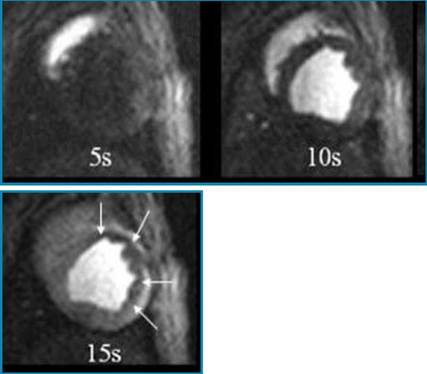
Fig. 4 Still frames in the short-axis view extracted from dynamic first-pass myocardial perfusion imaging, acquired 5,10 and 15 s after gadolinium injection, showing the distribution of contrast agent from RV (5 s) to LV cavity (10 s) and ultimately within the myocardium (15 s). Microvascular obstruction is displayed as hyposignal in the anterolateral wall (arrows) in this 53-year-old male who suffered acute MI and underwent successful angioplasty of the left anterior descending 48 hours before
ST elevation acute coronary syndromes [15]. Direct high-resolution CMR imaging of MI with the so-called “delayed-enhancement technique” after Gadolinium contrast injection is well standardized and carries important clinical implications for the diagnosis of myocardial viability [16]. With this imaging sequence, Gadolinium-DTPA enhanced imaging provides great contrast and high resolution images in which the infarct appears as a hyperenhanced region
relative to noninfarcted tissue on inversionrecovery images acquired 10-15 min after contrast injection (Fig. 5). Indeed, the differences observed after MI in myocardial wash-in/wash-out kinetics of Gadolinium enable to differentiate three patterns [14]: normal nonischemic myocardium is characterized by rapid wash-in of the contrast agent on first-pass images (30 min) due in a large part to an increase of the distribution volume.
Therefore, and because of greater Gadolinium content, the signal is enhanced (bright) on delayed images as compared to noninfarct- ed tissue.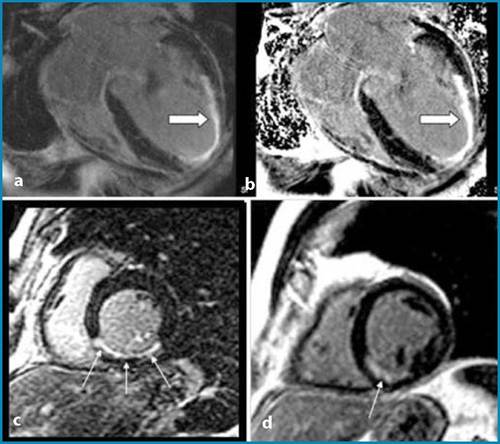
Fig. 5a-d Late inversion-recovery Gadolini- um-enhanced CMR images in the four- chamber view (a-b) showing late hyperenhancement of the apex and apical septum (arrows) at day 3 in a HIV infected patient who presented acute anterior MI. The infarct is transmural at the apex and subendocardial at mid-septum. c-d Late inversion-recovery Gadolinium-enhanced CMR images in the short axis view in a HIV infected patient who presented inferior MI, showing subendocardial late hyperenhancement in the posterior wall (arrows) at day 2
The third pattern corresponds to microvascular obstruction when perfusion is not adequate at the tissue level despite reopening of the culprit coronary artery. In this case, gadolinium wash-in is dramatically delayed and the signal is very low (black) on first-pass myocardial perfusion images relative to noninschemic or necrotic but reperfused myocardium. It is well established from contrast-echocardiography and contrast-enhanced CMR that microvascular obstruction identified at the tissue level during the days following MI is a predictor of poor outcome and adverse LV remodelling [17, 18]. Delayed-enhanced CMR has important clinical implications for detection of infarct size, which is the strongest determinant of prognosis in these patients, and for detection of myocardial viability [16]. Infarct imaging by CMR is very sensitive and can depict subtle non-transmural infarcts or even infarctlets [19, 20]. The method has been validated against PET for detection of viability and has been recognized as the standard of reference for viability detection by the ESC Consensus Panel report [21, 22].
Finally, common features of infarct imaging by CMR are characterized by the presence of delayed enhancement of the infarct- ed tissue, which occurs in a specific coronary territory and predominates in the subendocardium. The delayed-enhancement within the infarcted myocardium corresponds typically to a single area of hypersignal that extends towards the subepicardium as a wavefront. These patterns are observed in recent, as soon as a few hours after the onset of MI, and in chronic MI. The transmural extent of MI serves as an index of tissue viability, with graded probability of subsequent recovery after revascularization for a given myocardial segment that is inversely proportional to the initial transmural extent [16].