CMR of Myocarditis
Histopathologic evidence of myocarditis has been found in more than one-third of AIDS patients at autopsy, but no specific cause was identified in more than 80% of the cases [23].
Common pathogens found in patients with AIDS-related myocarditis include Toxoplasma gondii, Mycobacterium tuberculosis, and Cryptococcus neoformans. Other infective agents that have been reported are M. avium-intracellulare complex, Aspergillus fumigatus, Candida albicans, Coccidioides immitis, cytomegalovirus, herpesvirus types 1 and 2 [24, 25], and Chagas disease in South America. HIV itself has been implicated as a cause of myocarditis. Since cardiac myocytes do not possess CD4 receptors that would allow a virus to enter the cell, it is not clear how a virus gets into the myocytes. Reservoir cells (dendritic cells), along with infection and injury of myocytes by cardiotropic viruses, may facilitate the entry of HIV into CD4 receptor-negative cells [26-28]. Lymphocytic myocarditis was present in almost 50% of patients who died of AIDS [23], and it is frequent in patients with LV dysfunction [29, 30]. Autoimmune abnormalities and nutritional deficiencies have been implicated in AIDS-related myocardial disease, and cardiac-specific autoantibodies such as antimyosin, have been found in 30% of patients with HIV-associated cardiomyopathy [31]. An association between the use of zidovudine and cardiomyopathy also has been reported [32]. Myocarditis corresponds to an acute aggression of the myocardium, resulting in various degrees of myocyte necrosis associated with cellular infiltration, inflammation, and edema [33-35].In contrast to MI, myocyte necrosis preferentially occurs in the subepicardial layers and tends to diffuse inward transmurally during the course of the disease. The myocardial areas involved by the pathologic process do not correspond to any predefined coronary territory.
In approximately 10% of the cases, acute myocarditis can lead to acute heart failure. It may also have subacute course such as rapidly progressive dilated cardiomyopathy with subsequent heart failure. The disease can evolve to chronic features and persistent dilated cardiomyopathy. Acute myocarditis can also be revealed by an acute chest pain mimicking ST-elevation or non-ST-elevation acute coronary syndrome. In both cases, troponin I measurements may be increased. The presumed diagnosis of myocarditis is often difficult to confirm. The clinical presentations, ECG, laboratory tests, and echocardiography are not specific. Coronary angiography may serve to eliminate an unstable coronary stenosis. Endomyocardial biopsy is the most specific examination and has been considered as the method of reference. In clinical practice, it is often skipped because of its invasive property and low sensitivity, estimated in the range of 50-65%, due to the patchy and heterogeneous distribution of myocardial tissue damage [35, 36]. The sensitivity of 67Gallium myocardial scintigraphy is relatively poor [35, 37]. Myocardial scintigraphy with 111Indium-labelled antimyosine monoclonal antibodies, which are fixed specifically to intracellular myosine within the damaged cells, carries higher sensitivity but low specificity [36, 38]. Therefore, the need for a reliable diagnostic tool is of great importance.Several preliminary studies have shown the capability of CMR to image myocardial damage during the course of acute myocarditis [39, 40]. One of the main interests of this technique relies on its sensitivity to rapid changes in tissue composition and its ability to visualize the entire myocardium, which is required for the accurate detection of a patchy and sometime diffuse inflammatory pathologic process [33, 41]. The comprehensive CMR examination is well standardized and quite similar to that used in particular for the evaluation of ischemic cardiomyopathy and viability assessment [42, 43].
It includes steady-state free precession cine-CMR for assessment of LV function, pre-contrast breath-hold ECGgated black-blood T2-weighted sequence, dynamic first-pass perfusion myocardial imaging during the minute following 0.05-0.1 mmol.kg-1 Gadolinium chelate injection, and delayed-enhanced T1-weight- ed imaging with inversion-recuperation 10 min after injection.CMR features vary according to the time elapsed from the onset of symptoms to the time of the CMR study. Although still debated, one can schematically distinguish a focal form of acute myocarditis within the first 5 days that may evolve towards a more diffuse process [33, 44, 45]. CMR is able to detect ongoing inflammation, its extent and severity, and to differentiate myocardial involvement from that of acute or chronic MI [46, 47]. It may also depict myocardial damage as sequelae of a previous episode of myocarditis when fibrotic scar tissue is present. During the first days of the disease, myocardial edema is present in about 30% of cases and appears as a hypersignal on T2- weighted images (Fig. 6). Edema involves predominantly the inferolateral wall with or without increased wall thickening. Pericardial effusion is noted in approximately 20% of cases and generally moderate. Cine-CMR may reveal wall motion abnormalities that may be segmental or more diffuse. In the most severe forms (fulminant myocarditis), LV ejection fraction is severely depressed without LV dilation. Segmental wall-motion abnormality may be present in myocardial segments that can be different from those exhibiting myocardial damage on delayed enhancement sequence.
In contrast to microvascular obstruction frequently observed after acute MI, there is
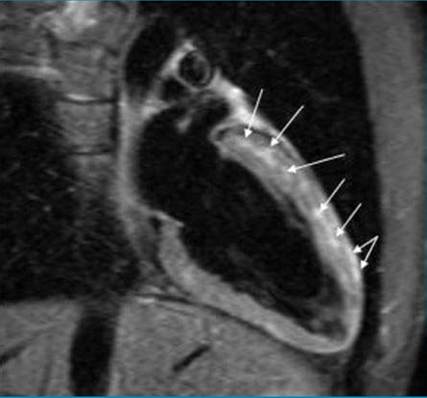
Fig. 6 Non-contrast black-blood ultrafast spin echo T2-weighted image in the 2-chamber view, in a 31- year-old HIV-infected male with acute myocarditis (day 2), showing multiple nodular and linear foci of hypersignal in the anterior wall that predominate at midwall and in the subepicardium (arrows).
These patterns that occur most frequently in the inferolateral wall are very specific of viral acute myocarditisno perfusion defect on contrast-enhanced first-pass perfusion imaging [47, 48]. Conversely, areas of delayed contrast-enhancement are frequent, either nodular predominating in the subepicardium or showing up as linear bands preferentially at mid-wall (Fig. 7). Myocyte membrane rupture leading to increased extracellular space, edema related to the inflammatory phenomenon with capillary compression, increased vascu-
lar permeability responsible for an increased distribution volume, along with decreased Gadolinium clearance may explain Gadolinium accumulation in regions involved in the pathologic process of acute myocarditis. These lesions occur in the same territory as edema and do not correspond to a specific coronary territory. These abnormal areas of delayed-enhancement are very often localized in the inferolateral wall.
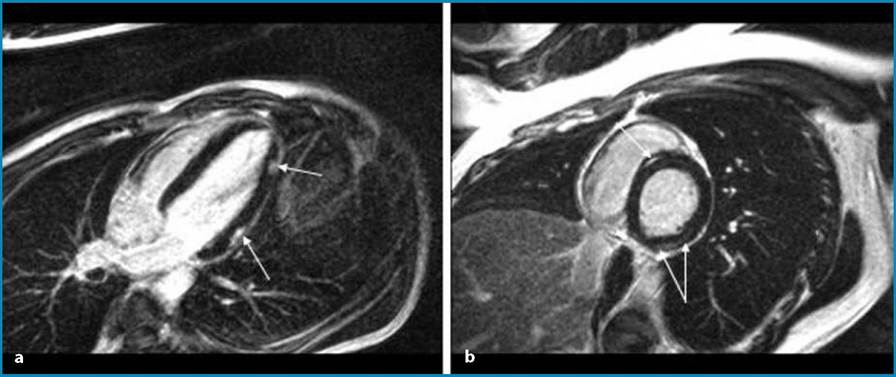
Fig. 7a, b Delayed contrast-enhancement CMR images obtained in the four-chamber (a) and the short-axis views (b) in a 34-year-old male with HIV infection, presenting with acute myocarditis at day 3, and showing nodular foci of hyperenhancement in the subepicardium of the lateral wall (a, arrows) and linear bands at mid-wall in the inferolateral and anteroseptal walls (b, arrows)
More subtle patterns such as micronodu- lar lesions can be observed. These abnormal delayed-enhancement patterns have low sensitivity (around 60%) but a high specificity (97-100%), underlining the crucial need of performing a comprehensive CMR examination using a combination of different imaging sequences to improve diagnostic accuracy [43, 47, 48]. After 10 days, subacute forms are more difficult to pick by CMR because of the diffusion of the viral process in the myocardium [33, 39, 44, 45]. The edema is less important and more diffuse such as wall-motion abnormality. Delayed- enhancement may be difficult to highlight because of a more diffuse process. Specific outcome data in HIV infected patients are missing. Several longitudinal studies have followed non-HIV patients up to 3 months [39, 44, 49]. A favourable outcome was observed when LV contractile function improved and paralleled a significant decrease or involution of damaged delayed- enhanced myocardial tissue. Although still controversial, early hyperenhancement occurring a few minutes after gadolinium injection at the acute phase and persisting up to 1 month after the onset of symptoms could be indicative of poor outcome.