Coagulative Disorders in HIV-Infected Patients Leading to Thrombotic Conditions
Coagulative Disorders in HIVPatients Undergoing HAART and Arterial Risk of Thrombosis
Emphasis has been placed on the deleterious associations/consequences of coagulative disorders and the two main high cardiovascular risk conditions of HIV patients undergoing highly active antiretroviral therapy (HAART): the metabolic and lipodys- trophic syndromes.
These conditions are associated with an overwhelming risk of cardiovascular events among the numerous metabolic and hemostatic pathways that are modified in these conditions: the coagulative systems and mostly the fibrinolytic systems are affected. The best-documented coagulative abnormalities associated with these conditions are an increase of plasminogen activator inhibitor-1 (PAI-1) and a decrease of fibrinolytic potential.Coagulative Disorders in HIV Patients Undergoing HAART Linked to the Increased Risk of Cardiovascular Disorders
Hypofibrinolysis is associated with insulin resistance in HIV-infected patients receiving HAART, especially in those with metabolic syndrome.
The levels of PAI-1 and fibrinogen are significantly increased in patients receiving protease inhibitors (PIs) compared with control subjects, independently of HAART- associated metabolic syndrome. PAI-1 — and tissue plasminogen activator (tPA) — levels have been shown to be independently correlated to the use of PIs, triglyceride and insulin levels, body mass index, and gender in several studies (Fig. 1) [1]. Metformin treatment induces an improvement in PAI-1 levels. Changes in insulin AUC correlate significantly with changes in tPA antigen concentration. By reducing PAI-1 and tPA antigen concentrations, metformin may ultimately reduce the cardiovascular risk in patients with fat redistribution and insulin resistance [2].
Plasma PAI-1 concentrations are increased in direct proportion to liver fat content in HIV patients with lipodystrophy receiving HAART.
Rosiglitazone decreases liver fat content, serum insulin, and plasma PAI-1 without changing the size of other fatHAART Naive
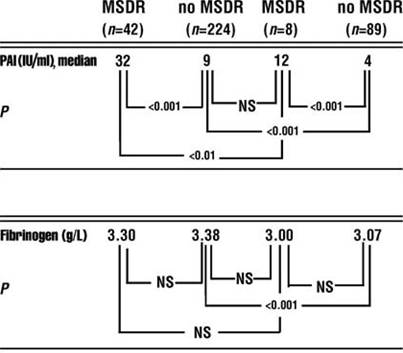
Fig. 1 Levels of plasminogen activator inhibitor type 1 (PAI-1) and fibrinogen in HIV-1-infected patients receiving protease inhibitor-containing higly active antiretroviral therapy (HAART) and treatment-naive HIV-1-infected patients with and without metabolic syndrome (MSDR) at the time of the cross-sectional study. NS, not significant. (From [1], with permission)
depots or PAI-1 mRNA in subcutaneous fat. These observations suggest that liver fat contributes to plasma PAI-1 concentrations in these patients (Fig. 2) [3].
HAART Reduces Markers of Endothelial and Coagulation Activation in HIV-1-Infected Patients
Endothelial-derived proteins — soluble vascular cell adhesion molecule-1 (sVCAM-1), soluble intercellular adhesion molecule-1 (sICAM-1), and von Willebrand’s factor (VWF) — are markers of endothelial lesion and/or activation. These markers are increased in HIV-infected patients and they are usually considered as markers and/or agents of the accelerated atherosclerosis which characterizes HIV-infected patients independently of HAART and HAART-asso- ciated metabolic syndrome. The increased plasma level of VWF [4] could be related to the inflammatory status, to antiretroviral treatment, but also to the direct lesion of
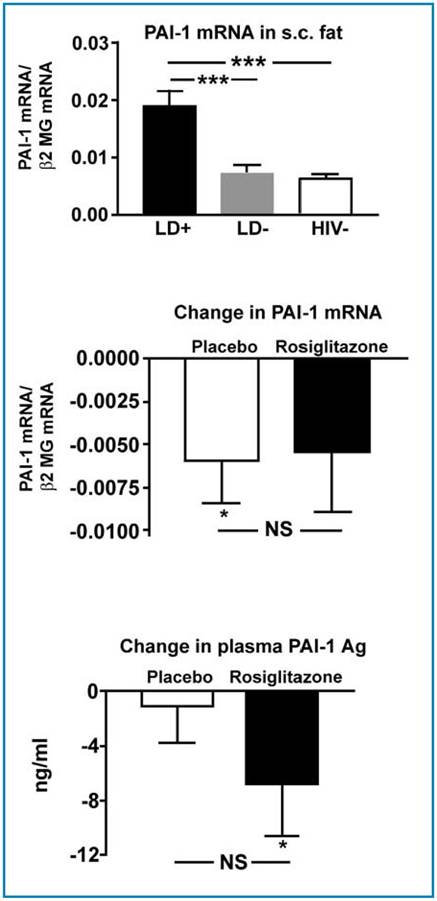
Fig. 2 PAI-1 mRNA expression in subcutaneous (s.c.) adipose tissue (top) and the change by rosiglitazone versus placebo treatment in PAI-1 mRNA (middle) and plasma PAI-1 antigen concentration (bottom). LD+ indicates HIV+ patients with HAART-associated lipodystrophy; LD-, HIV+ patients using HAART but without LD; HIV-, HIV- normal subjects; b2 MG, b2-microglobulin. NS, not significant.
*pbgcolor=white>sP-selectin, ng/mlMost of these factors are correlated with each other [34] and with the markers of activation of the coagulation/fibrinolysis reaction (such as the D-dimers), with the status of immunodeficiency, with opportunistic infections, with cancer complications, and with the inflammatory status.
Three different types of mechanisms of VTEE linked to treatments can be differentiated:
- Those due to the central catheters required in patients with severe undernourishment [49]. It seems that among HIV-infected patients requiring total intravenous nutrition, a low-dose oral anticoagulant regimen does not have the efficacy encountered in other types of patients treated with a central catheter [50].
- Those related to the administration of megestrol acetate [35].
- Those related to PIs [18, 51]. This observation is in apparent opposition with two other types of observations on PI-related effects in HIV-infected patients:
- Effective antiretroviral treatment in HIV-infected patients decreases markers of endothelial activation/lesion [5] and markers of coagulation activation [6].
- Antiretroviral treatment exerts a prohe- morrhagic effect in hemophilic patients infected by HIV-1 [52].
Treatment-Related VTEE in HIV-infected Patients
PIs are large lipophilic molecules metabolized by P450 cytochromes. The same P450 cytochrome system also metabolizes oral anticoagulants (warfarin) [53]. HIV-infected patients often have complex clinical signs such as thrombocytopenia or other clinical manifestations or treatment which often represents a contraindication to warfarin treatment so that other types of therapy may be required such as the use of low- molecular-weight heparin for long periods.