Death and dying
When treatment is futile, persevering with treatment and investigation can be obstructive in allowing a patient a dignified and meaningful death. The patient should be at the centre of the decision-making process as much as is possible.
It is at this time that the multiprofessional team is so important.Facilitating choice
If you have been managing your patients properly and involving them in decision-making, the groundwork for managing the last weeks or months should have been done, you will have a good enough relationship to be honest and open and to finish these last preparations. If you have not faced these with your patient in some form, even by flagging that “a time will come^” whilst not failing them as a technician, you will have failed as a doctor. This is the time to check regularly about a patient's wishes. Proper links and services from primary care and social services are essential and friends, family and professionals should be as much “in the know” as possible.
Two additional symptoms
Movement-related pain
This is a common problem in dying patients with HIV and is best managed with NSAIDs. If the patient cannot swallow, then rectal indometacin is very effective.
Box 14.13 Preparing for death
• Do they want active treatment if they deteriorate? If so, what level of resuscitation do they want? Is there a time or circumstances in which they wish treatment to be withdrawn or withheld?
• Will they feel more in control if these are written formally? A ‘Living Will’ or Advance Directive can be of great help to some patients by ensuring that their wishes are known if they become incapable. (See the BMA guidelines “Advance Statements: a guidance to practitioners”.)
• Have they said their goodbyes, sorrys and thank yous?
• Are there remaining personal matters to address: a will, funeral preparations, etc?
• Do they want to be at home? If so, is it suitable?
Pulmonary secretions
Retained secretions in patients too weak to clear them can be controlled with hyoscine 0.6-1.2mg s.c.
over 24h or glycopyrronium 0.6-1.2 mg s.c. over 24hours. If they fail to clear, use furosemide (frusemide). Reassure family that noisy breathing of itself is not distressing to the patient.As death approaches
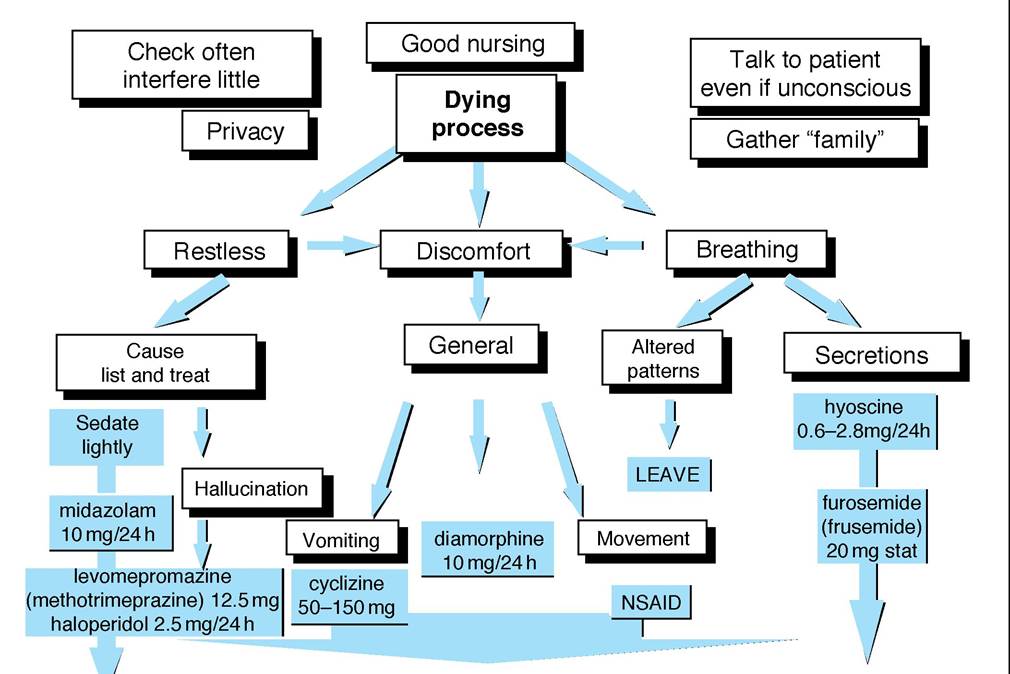
In the last days of life, pragmatism and sensitivity are essential. Patients have no appetite, are weak and somnolent or unconscious. Altered breathing patterns can last for days. Be calm and reassuring: relieve anxiety for both patient and carers by explanation that these changes are normal and don't cause physical suffering, which is true.
Most importantly continue to visit. The clinical situation can change very quickly. Assess symptoms regularly and change palliative therapeutics as necessary (even several times a day). As swallowing becomes difficult swap to parenteral routes. Most drugs for symptom control can be given continuously via a syringe driver subcutaneously. (Drugs can be mixed, see the charts in Twycross et al. 1998.) Figure 14.5 summarises management in the last few days of life.
With the limited communication, problems may manifest themselves as pre-terminal restlessness or distress. Possible physical and psychological/spiritual triggers need to be checked and acted on.
In general encourage the family to talk normally to the patient and to say whatever they need to say. Reassure them that the patient can hear and continue to explain all that you do to the patient and chat normally through procedures. This period of life, when the dying process is actively underway, may be short lived or take many days. In most cases we do not know what is taking place. Where beliefs are unknown or unfamiliar it is best presented neutrally as a time of transition; when our place is to care.
Box 14.14 Pre-terminal restlessness
• Exclude urinary retention
• Treat any suspected pain
• Check that there is not an important visitor that the patient must see or hear
• Check for an important date or anniversary
• Exclude any important religious rite
• Sedate as necessary; midazolam (starting at 10mg/24 h), levomepromazine (12.5-300mg∕24 h).
advice TITRATE TO COMPLETE CONTROL REGARDLESS OF DOSE
Figure 14.9 Pain management in the last few days of life
It is important to allow those with religious beliefs the opportunity to see their advisors and perform necessary rituals as they wish. This can often lead to conflict if partners and family are of differing opinions. Give time to friends and family to spend talking over what has happened. Obviously you must be aware of the dynamics of the group and you must respect the patient's confidentiality.
Finally, a death affects us and the team involved. Debriefings and supervision work either individually or as a team can be most beneficial.