Symptom Control
General points
The significance of symptoms
Noxious and debilitating symptoms, and pain in particular, can destroy ones quality of life sufficiently to be significant risk
factors for depression and suicide irrespective of whether they are from a disease or its treatment.
Symptom control is an essential part of curative treatments.Interventions may not be conventional, for example using a drug for its side-effect rather than its accustomed indication (for example, opiates for breathlessness), or working psychologically with a patient's perceptions to alter a symptom's impact or its threshold. This idea of a symptom threshold or altering perception may be unfamiliar, but it holds the key to effective symptom control.
Thresholds
Symptoms only become problematical when a threshold is passed and one perceives there to be a problem. Anything that changes perception generally (fear, anxiety, etc.) can also alter symptomatology — information (bad news, unexpected deterioration, a new complication etc.) or feelings that are unwanted (fear of failing health, death, guilt, anger, bitterness, etc.) are all examples.
Non-medical symptom control
Equally, symptom thresholds can be raised by psychological interventions and measures that calm, allow patients to unwind or promote a coping mechanism. For example aromatherapy and other complementary therapies, meditation and prayer are effective for some. Massage and acupuncture have solid evidence to support their effects on musculoskeletal and myofascial pain, as do breathing exercises and respiratory pacing in breathlessness. Diet is obviously important in nausea, vomiting and bowel control.
Pain management
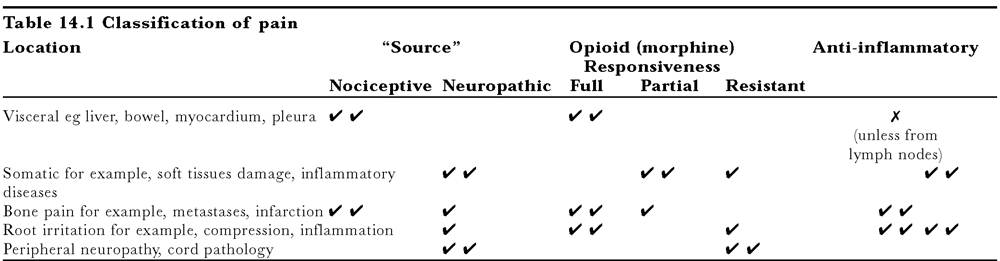
Pain is what the patient says it is. Leaving emotion and “soul” for the moment, pain can be classified in several different ways (Table 14.1). This is simplistic, but practical.
Nociceptive pain is usually opiate sensitive and neuropathic pain is opioid resistant.Evaluating pain
Over 90% of pains are controllable. All pain can be improved. Take a proper history and examine the patient to establish exactly what is going on.
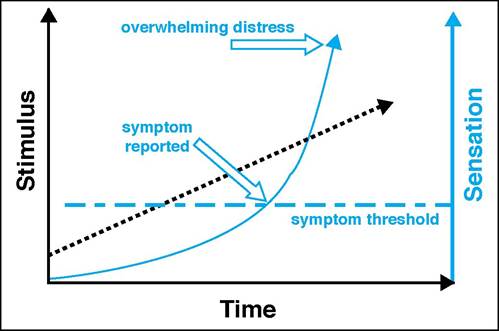
Figure 14.3 Sympton thresholds: the relationship between a noxious stimulus (for example, pain) and the reported symptom is exponential. Once past its threshold, without adequate treatment or a reduction in the process, the symptom will soon become intolerable. If the patient's threshold falls, the symptom will escalate in the same way, even when the underlying disease is stable
time
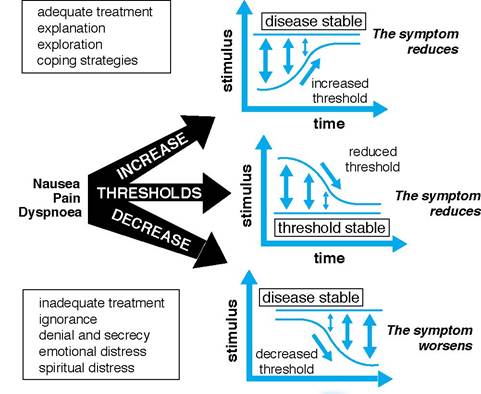
Figure 14.4 Sympton thresholds and what can change them
| Table 14.2 Drugs used in pain management | |||
| Weaker opioids | Strong opioids | Co-analgesics | Non-opioids |
| DHC | Oramorph | Anaesthetic agents | Muscle relaxants |
| Codeine | Diamorphine | Anti-convulsants | NSAIDs |
| Tramadol (?) | Hydromor phone | Anxiolytics | Paracetamol |
| Co-proxamol | Fentanyl | Corticosteroids | COX2 inhibitors |
| Oxycodone (also used | Dextromoramide | Tricyclic antidepressants | |
| as strong opioid) | Dipiponone | ||
To be able to monitor the pain it must be recorded accurately. Use body charts to localise the pain and get an estimate of each element of the pain by asking to score or grade the pain as a score out of 10 for intensity (0 = no pain, 10 = the worst pain you could imagine).
This will help in monitoring treatment, but it will also give the patient a sense that pain is not fixed and can improve.Box 14.5 Fundamentals of pain management
• Any pain, however generated, is a genuine symptom
• Always assume that there is a physical trigger, until proven otherwise
• The vast majority of patients have a combination of pain types
• The correct dose of an analgesic is that which relieves the pain
Opiates and nociceptive pain
Nociceptive pain is managed by using the World Health Organization (WHO) analgesic ladder. Over 90% of such pains are controllable in this way.
When prescribing any opiate, nearly all patients need a laxative and nearly 50% need an antiemetic.
Bottom rung: Paracetamol influences other drug's metabolism. However, in general, palliative physicians use doses up to 6g a day. Similarly gastrointestinal complications (with appropriate prophylaxis) or renal impairment with NSAIDs are not absolute contraindications in patients with a short prognosis and severe pain.
Middle rung: The weak opiates, or compound analgesics (co-codamol, co-dydramol, etc.), may be helpful for mild to moderate pain. Formulations differ slightly in efficacy and prescribing is empirical. Low-dose strong opioid can be used. Dependency is less than 0.1%.
Upper rung: Many strong opiates are available. Morphine is the drug of choice by mouth. Use other opioids only where there is a specific problem with morphine. Alternatively using co-analgesics may reduce side-effects.
Box 14.6 Morphine facts
• Dose range is 1000-fold, (2.5 mg 4-hourly to 2.5 g 4-hourly or more)
• Most patients require less than 200 mg morphine equivalent per day
• It is not addictive when used therapeutically
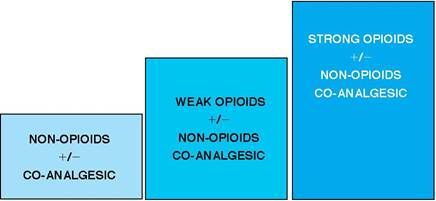
Figure 14.5 The WHO analgesic ladder
Box 14.7 Opioid side effects
• Nausea and vomiting — dose related
• Constipation — may be desirable, dose related
Peripheral effect Always prescribe laxatives
• Clouding of consciousness — hallucinations rare
Central effect, fades with time Warn the patient of initial drowsiness
• Respiratory depression — good for dyspnoea
Central + peripheral cough suppression Pain has a partially protective effect Increase dose carefully where chronic lung disease present
• Itch — histamine release
Opiate toxicity
Toxicity is idiosyncratic and dose dependent.
For some the therapeutic window may be very small. In poorly controlled pain (usually non-opioid responsive), escalating doses may lead to toxicity: confusion, hallucinations, agitation and myoclonic jerks. Paradoxical pain (loss of analgesia and increasing pain) may occur.Confusion in the dying is complex and increasing opiates is not the only solution to increasing pain. You may need to stop all opiates until symptoms have subsided. Seek the advice of an expert
Good prescribing
Opioid responsive pain can normally be controlled within
24— 48 hours. Morphine should be titrated using immediate- release formulations (Oramorph elixir, Sevredol tablets). Their effect peaks within the hour and last four hours. Titrate with a four-hourly regimen with “top-ups” for breakthrough pain of
25— 50% dose and a 25—50% increase in the next scheduled dose as necessary. In individuals with hepatic or renal impairment the increases should proceed more slowly. Slow-release preparations (for example, MST b.d. or MXL o.d.) are best for maintenance. Immediate release formulations should continue to be available for breakthrough pain at a dose at least one-sixth the final 24-hour dose.
Box 14.8 Dealing with opiate toxicity
• The half-life of morphine and diamorphine is four hours
• Respiratory rates down to 5 or 10 are acceptable for a few hours
• Central effects can be antagonised, but will lead to rebound agitation and hyperresponsiveness
• It is best simply to stop the opiate and wait
• In extremis: naloxone is the specific antidote and reverses all the actions of opiates. Use very small doses
• Physostigmine can be used to selectively antagonise respiratory depression
Box 14.9 Prescribing for nociceptive pain
• By the ladder:
Don’t forget that co-analgesics and non-opioids should be added to what you already use
• By the clock:
NEVER use prn pain control for example, 4-hourly for morphine liquid, 12-hourly for MST
• By the right route:
Use the mouth where possible, parenteral drug is no more effective
Opioid non-responsive pain
Neuropathic pain: Drugs affecting nerve conduction or central processing usually work.
Regimens are empirical as the numbers needed to treat (NTTs) between groups are similar; benefit may take several days to gain; neuropathic analgesics have significant side-effects and dose increases should be made slowly. Patient, family and staff may need support in keeping a steady hand whilst the best combinations are found.Intractable cases or root or cord problems (for example, CMV) may need a nerve block or long-term epidural. Many different techniques are available. They carry potential morbidity, so use cost-benefit analysis with the patient to decide a plan. Do not make choices on behalf of the patient; immobility and incontinence free of pain may be a valid choice.
Compound pains: Many patients have pain from tissue damage and the nervous system simultaneously. Their treatment requires accurate diagnosis and specific co-analgesics. Morphine may play a part in their management. To read more on this see Further reading on page 95. Make a habit of enlisting specialist support with neuropathic and compound pains.
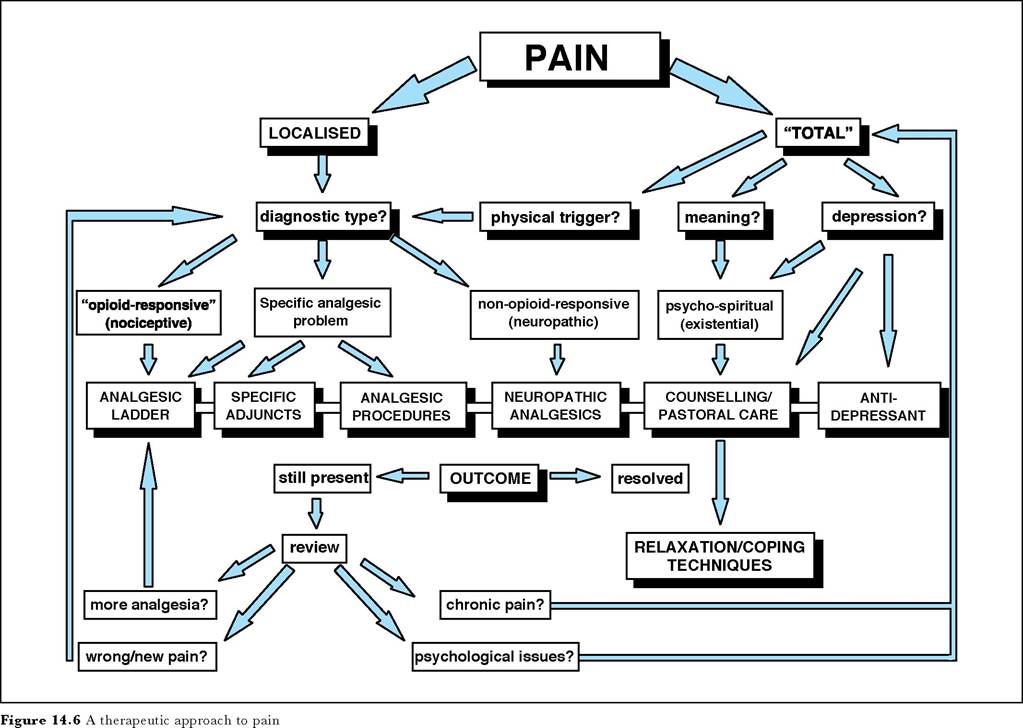
Total body pain and suffering
This is the difficult area of suffering and the subtle interactions of our psyche, beliefs and body. Some people use the terms “soul”, spiritual, or “emotional” pain. It is complex, distressing and very real (Fig 14.6). It stems out of a lowered threshold of distress and may occur with other symptoms as well. For understandable reasons, there is always an element of this in any dying person as they process and face their death and what it means. Fear and guilt are the common roots for many. Don't forget, paene (punishment) is the Latin root of pain.
Box 14.10 Neuropathic pain
• Generated in nervous system
• Source can be local nerve to thalamus
• Caused by:
Toxins for example, chemotherapy Invasion/compression, for example, by tumour Damage by viruses for example, HSV, CMV, HIV Demyelination of any kind
Often coexists with nociceptive pain
May not present with classical dysaesthesia
• Seldom opioid responsive
Box 14.11 Neuropathic analgesics
• Tricyclic antidepressants:
Lofepramine (70mg 1-3 times/day) or Amitriptylline (10-150mg nocte +/- day time doses)
• Anticonvulsants:
Gabapentin (start dose of 300mg up to 2700mg) Carbamazepine (100mg b.d.
up to 1600mg per day), Valproate (ranging from 200mg to1200mg per day) Phenytoin (up to 300mg per day).• Benzodiazepines:
Clonazepam (0.5-4 mg nocte), Diazepam, midazolam (parentally)
• Membrane stabilisers:
Flecainide (100-200 mg b.d.),
Lidocaine (lignocaine) (subcutaneous or i.v. infusion in doses of 0.5-2 mg/kg/h)
• Others:
Clonidine, octreotide, etc. seek advice
Effective management requires one to deal not only with any physical component, but also with the meaning of the symptomatology and the exacerbating effects of fear, anxiety, sleeplessness, loss of future, and of death and its connotations for the individual. In this difficult area do not be afraid to refer for help from a counsellor, psychologist or spiritual adviser.
Nausea and vomiting
These are the second most common symptoms, not least because of the burgeoning numbers of drugs that have gastrointestial side-effects. Careful assessment should ensure a logical and methodical use of antiemetics.
General guidelines
Nausea and vomiting is usually “uncontrolled” because of erratic and illogical prescribing in inadequate doses given orally. These guidelines are therefore common sense, but necessary.
Assess nausea and vomiting separately. Nausea tends not to respond to prokinetics. Treat any potentially reversible causes and stop emetogenic drugs if possible. Anxiety exacerbates nausea and vomiting and may need specific treatment.
Box 14.12 Logical and methodical use of antiemetics
• One-third of patients require more than one antiemetic for satisfactory control
• Select the most appropriate drug for the putative cause
• Use regularly, at optimum dose
• Have a low threshold for parenteral routes
• Careful re-evaluation on a regular basis
• Use adjuvant drugs such as corticosteroids and antisecretory drugs
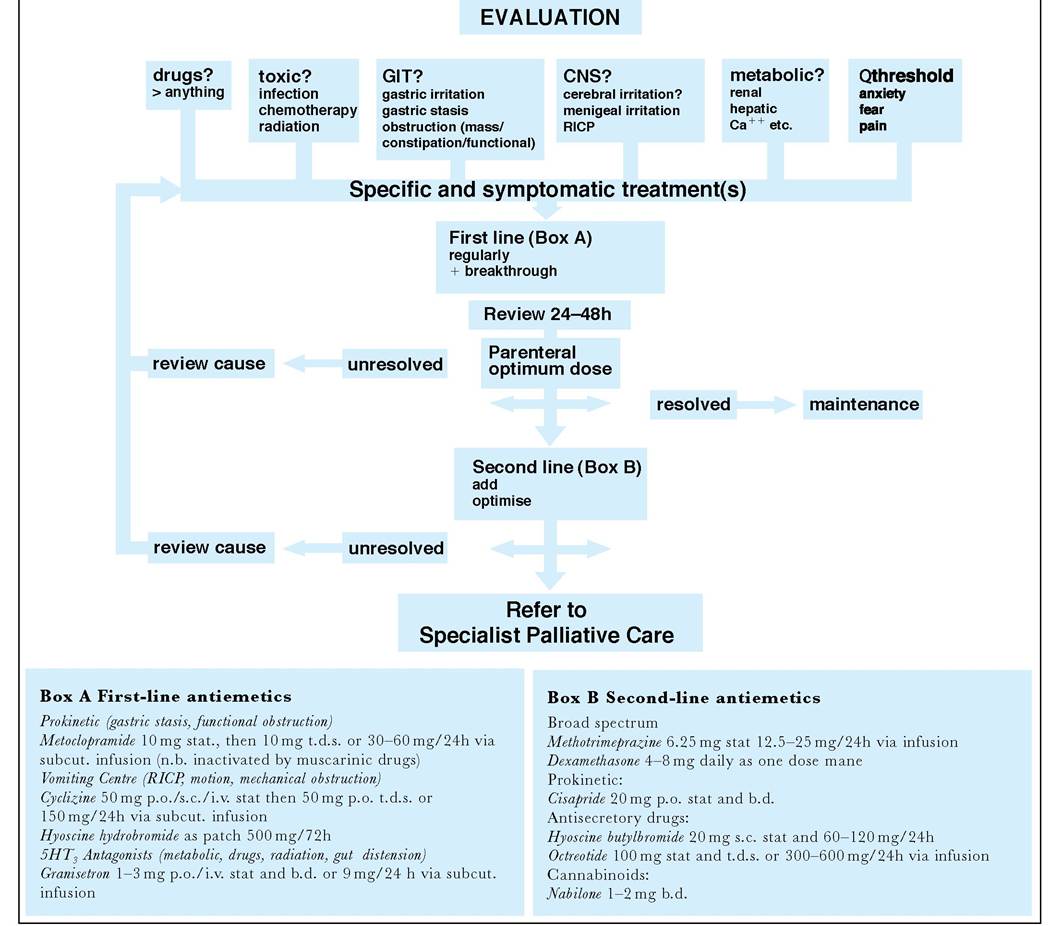
Figure 14.7 Guidelines for pain evaluation
Prescribe the most appropriate first-line antiemetic for the likely cause according to the figure. Prescribe both regularly and as required. If the patient is vomiting, or has been nauseous for some time administer parenterally, preferably by continuous subcutaneous or intravenous infusion preceded by a stat dose. Optimise the dose daily taking into account breakthrough doses and reported level of nausea and vomiting.
If there is no improvement, rather than changing the drug, optimise the dose, and re-evaluate the cause. It may influence your drug choice. After 48 hours, substitute or add an appropriate second-line, broader spectrum antiemetic. A significant minority of patients need more than one antiemetic. Consider non-drug treatments, including acupressure bands, control malodour, and ensure patient avoids foods that may precipitate nausea. If control remains poor, then refer. Only consider converting to equivalent oral regimen after 72 hours of good control and continue antiemetics indefinitely unless the cause is self limiting.
Other common symptoms
Other common symptoms are cognitive impairment, weight loss, malaise, weakness, pruritis, cough, diarrhoea, etc. Their differential diagnosis and appropriate investigations and management are covered more widely in the ABC of Palliative Care.
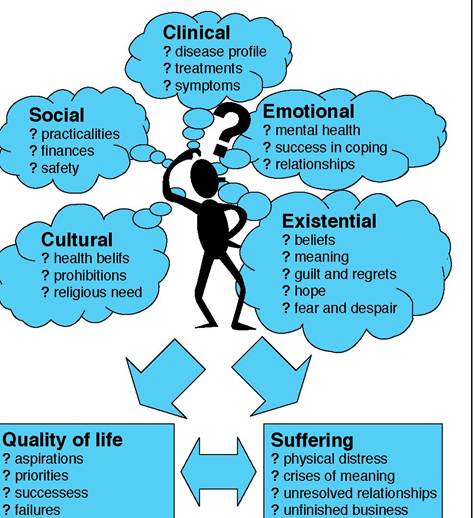
Figure 14.8 Aspects of palliative care: some elements necessary to holistic practice in chronic or progressive disease
More on the topic Symptom Control:
- Palliation and symptom control
- Pain control
- Social considerations
- 51 Palliative Care
- SELECTION PROCEDURES
- Crystalline Arthritis
- THE MILKING ROUTINE AND MASTITIS CONTROL
- Death and dying
- Faecal incontinence
- Management of gastrointestinal symptoms