Crystalline Arthritis
GENERAL PRINCIPLES
Definition
Crystalline arthritis is caused by deposition of microcrystals in joints and periarticular tissues. Common types of crystalline arthritis are gout, pseudogout, and apatite disease.
Gout
Gout is a monosodium urate crystal deposition disease. This can occur in joints (inflammatory arthritis), soft tissues (tophi), and kidneys. Is the most common form of inflammatory disease in men. Gout is uncommon in premenopausal women due to the uricosuric effect of estrogens.
GENERAL PRINCIPLES
Etiology
Gout is characterized by hyperuricemia that can be due to underexcretion or overproduction of uric acid.
• Overproduction: Primary: due to genetic polymorphisms associated with changes in uric acid excretion. Secondary: patients with psoriasis, myeloproliferative disorders, multiple myeloma, hemolytic anemia, and cytotoxic drugs. May also occur because of intake of purine-rich diet, alcohol, or fructose.
• Underexcretion: chronic kidney disease (CKD), lead nephropathy, hyperparathyroidism, hypothyroidism. Medications such as loop diuretics, thiazides, low-dose aspirin, cyclosporine, tacrolimus, niacin, and ethambutol all interfere with renal excretion of uric acid.
DIAGNOSIS
Clinical Phases
Natural disease history is divided into three phases.
• Asymptomatic hyperuricemia: defined as uric acid levels gt;6.8 mg/dL without arthritis or urate nephropathy. Usually present for many years prior to the first attack. The majority of the patients with asymptomatic hyperuricemia do not develop gout.
• Acute intermittent gout: acute attacks of arthritis followed by symptom-free intercritical periods.
• Chronic gouty arthritis: may occur in untreated patients. They experience pain during the intercritical periods between the attacks. Tophi, urate nephropathy, or uric acid stones may occur.
Clinical Presentation
• Acute gouty arthritis presents as an excruciating attack of pain. Characterized by sudden onset of pain, erythema, and swelling. Usually in a single joint of the foot or ankle although other joints may be affected. Inflammation of the first metatarsophalangeal joint called as podagra is a classic presenting feature of gout. Acute gouty arthritis attacks can be precipitated by surgery, dehydration, diuretics, fasting, binge eating, or heavy ingestion of alcohol.
• Chronic gouty arthritis: When left untreated the disease can progress to chronic gouty arthritis. It may cause a symmetric large and small joint involvement known as a pseudorheumatoid arthritis pattern.
Diagnostic Testing
• Hyperuricemia alone is not diagnostic.
• Serum uric acid level is normal in 30% of patients with acute gout.9
• Increased ESR and CRP.
• Synovial fluid analysis of the affected joint or bursa is the gold standard for diagnosing gout. A definitive diagnosis of gout is made by finding intracellular crystals in synovial fluid examined with a compensated polarized light microscope. Crystals can also be identified during the intercritical period in asymptomatic patients but are usually not intracellular. Urate crystals are needle-shaped and strongly negatively birefringent. Leukocyte counts are elevated, usually gt;15,000#8725;#956;L with neutrophilic predominance.
IMAGING
• Joint x-rays are normal early in the disease course. Later they may show punched-out joint erosions with overhanging borders. Tophaceous deposits may be visible in the soft tissues on x-rays.
• Ultrasonography can detect joint effusions, erosions, crystal deposition on the cartilage surface (double-contour sign), crystal aggregates in synovial fluid (snowstorm appearance), and tophaceous deposits.
• Dual-energy computed tomography (DECT) enables visualization and volume assessment of tophi.
TREATMENT
• Asymptomatic hyperuricemia is not routinely treated.
However, patients should be monitored closely for the development of complications if the serum uric acid level is at least 12 mg/dL in men or 10 mg#8725;dL in women. Lifestyle measures such as avoidance of alcohol and limiting intake of sugar and foods rich in purines should be discussed with all patients.î Management of gout includes symptom control with anti-inflammatories in acute gout flares, urate- lowering therapy (ULT), prophylaxis of mobilization flares, and management of risk factors.
Acute Gout Treatment
Although the acute gouty attack will subside spontaneously over several days, prompt treatment can abort the attack within hours (Table 25-2).
TABLE 25-2
ACUTE GOUT TREATMENT
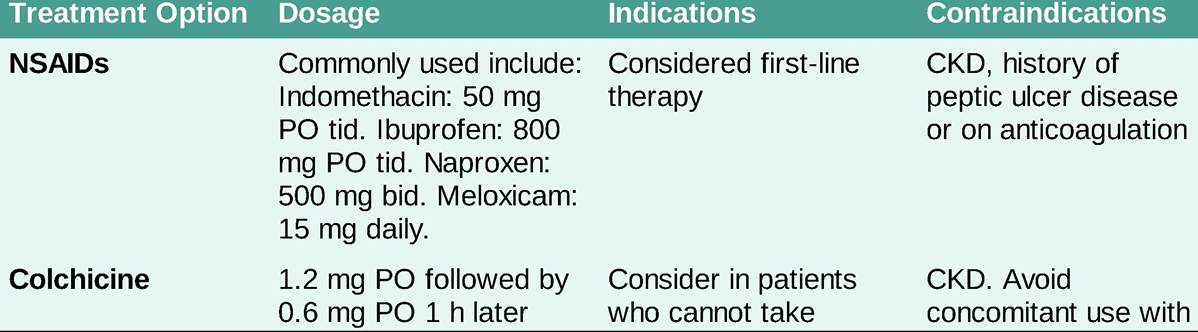
CKD, chronic kidney disease.
Urate-Lowering Therapy
• Indications: Indicated in patients with two or more acute gout flares a year, presence of tophi, urate nephropathy, or radiographic damage. In patients experiencing their first gout attack, ULT should be considered if uric acid is greater than 9 mg/dl, presence of nephrolithiasis, or if the patient has CKD #8805; stage 3.
• Uric acid level goal will depend on the presence or absence of tophi. If tophi are present, uric acid goal is lt;5 mg/dL, but if tophi are not present, uric acid goal is lt;6 mg/dL.
• Timing: ULT can be initiated at least 2 weeks after the attack subsides and while the patient has had at least 1 week of prophylactic therapy (reviewed below). If the patient is on ULT, do not discontinue it during an attack because any alteration in uric acid levels may worsen or prolong an attack. Once you reach uric acid level goals, ULT should be continued indefinitely (Table 25-3).
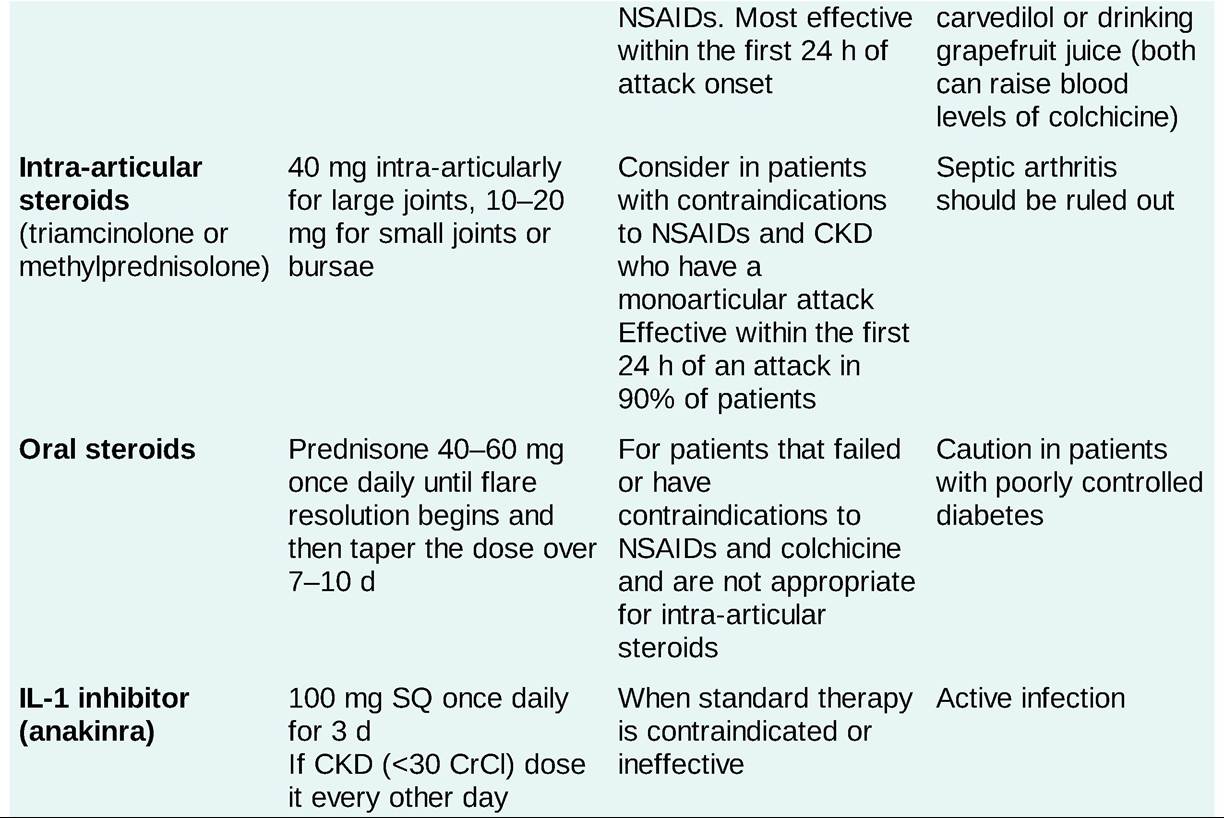
URATE-LOWERING THERAPIES

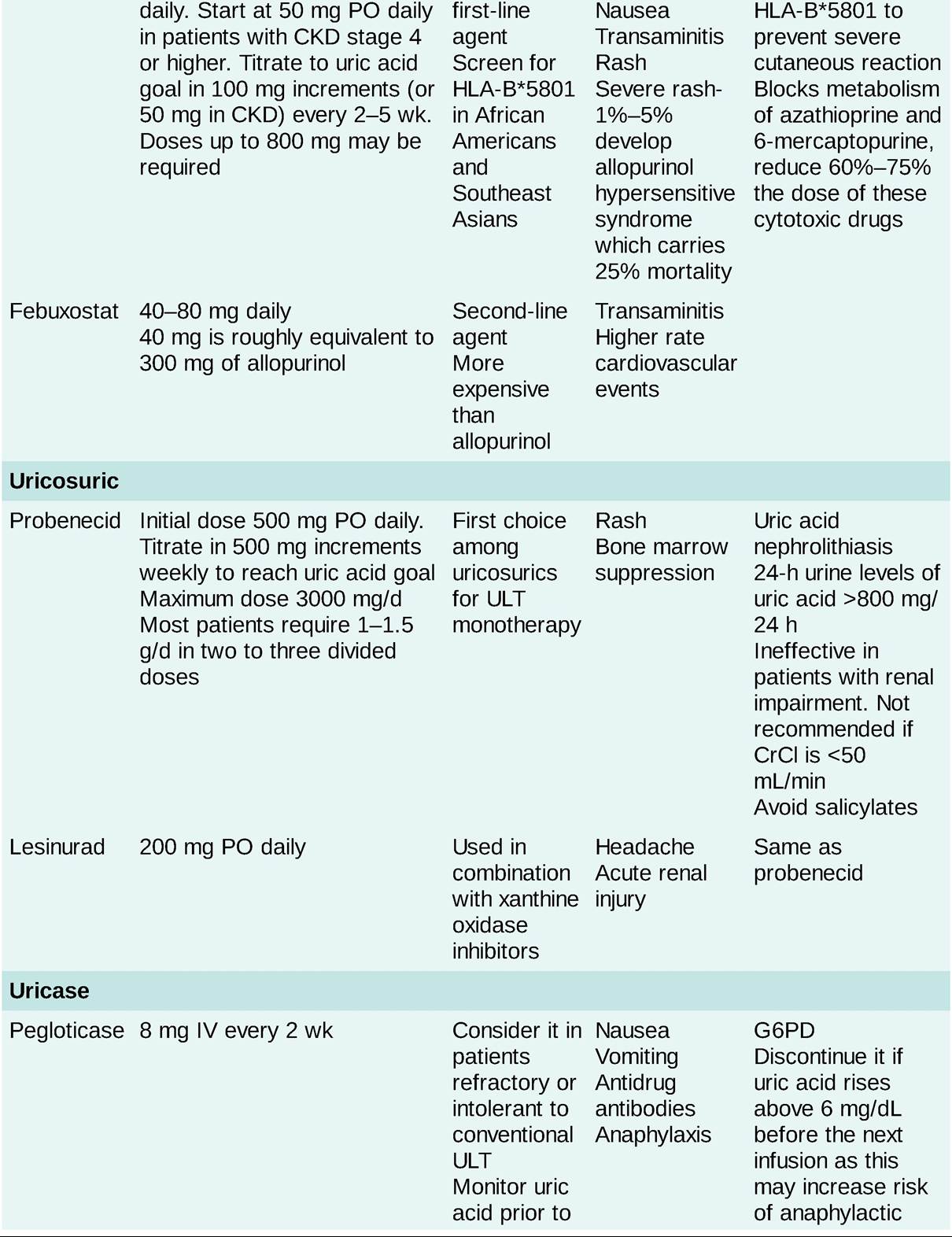

CKD, chronic kidney disease; ULT, urate-lowering therapy.
Prophylaxis of Mobilization Flares
Patients who are started on ULT will have uric acid mobilization which can precipitate acute gout flares. Prophylactic therapy should be given in patients starting ULT to prevent this. Options include colchicine 0.6 mg PO daily (consider every other day dosing in CKD and elderly) and low-dose NSAIDs. Low-dose steroids (i.e., prednisone 5-10 mg) can be used if the above are contraindicated.
Management of Risk Factors
• Dietary recommendations include weight loss, avoiding organ meats and food and beverages containing high fructose, and limiting the intake of beef, lamb, pork, shellfish, and alcoholic beverages (especially beer).
• Aspirin (uricoretentive) and diuretics should be avoided if possible.
More on the topic Crystalline Arthritis:
- Other Crystalline Arthritis
- Crystalline Arthritis
- THE CRYSTALLINE BODY OF LOGOS
- JUVENILE IDIOPATHIC ARTHRITIS
- Juvenile Idiopathic Arthritis
- Calcium
- PseudogoutZCalcium Pyrophosphate Deposition Disease
- Macrovascular Complications of Diabetes Mellitus
- Valproic Acid
- Amyloidosis and Amyloid-Like Nasal Deposition