Amyloidosis and Amyloid-Like Nasal Deposition
Amyloid (from the Greek amylon, “starch”) was so named by Virchow because it stained with iodine similar to that seen with cellulose. Amyloidosis is an important disease of laboratory mice, both as a spontaneously occurring, life-limiting disease and as an experimentally induced disease.
Amyloid is a chemically diverse family of insoluble proteins that are deposited in tissues but have in common a biophysical polymerized conformation known as the beta-pleated sheet. There are 2 types of amyloid in the mouse: AA and AapoAII. AA amyloid is associated with an increase in serum precursor apoSAA, which is induced in hepatocytes and elevated in blood in response to cytokines produced during inflammatory and neoplastic diseases. Local tissue injury elicits a complex of events in which macrophages release monokines, including interleukin 1 and tumor necrosis factor, which in turn stimulate apoSAA synthesis in liver. AA fibril formation and deposition involves partial degradation of apoSAA by macrophages. AA amyloidosis can be induced by repeated injections of casein and other inflammatory stimuli, thereby earning the name “secondary amyloidosis.” The spleen, liver, intestine, and kidney are the most common sites for AA amyloid deposition. Experimental secondary amyloidosis can be readily induced in a variety of laboratory mouse strains with casein injections. The order of susceptibility (in decreasing order) among common mouse strains is CBA, B6, outbred Swiss, C3H/He, BALB/c, and SWR. A/J mice are resistant. The second type of amyloid is AapoAII amyloid, which is also known as “primary” or “senile amyloid.” AapoAII amyloid consists primarily of apoAII proteins without degradation. The precursor apoAII is also produced by the liver. Mouse strains that are prone to AapoAII amyloidosis include A/J and SJL. AapoAII amyloid deposition tends to be less severe in spleen and liver (compared to AA amyloidosis), with more deposition in adrenals, intestine, heart, lungs, thyroid, parathyroid, ovaries, and testes.
In addition, a number of localized forms of amyloidosis occur, such as in endocrine tumors, ovaries, and the brain (in Alzheimer's disease), each with differing composition.Spontaneous amyloidosis is a common event in many strains of aging mice. It is difficult to distinguish between primary and secondary amyloidosis in spontaneous cases, since amyloid deposits are typically mixed, and patterns of tissue deposition may vary with mouse strain. Amyloidosis tends to occur at high prevalence and early onset in A, SJL, and outbred Swiss mice (mostly AapoII amyloid); high prevalence but late onset in B6 and B10 mice (mixed amyloid); and is extremely rare in BALB, C3H, and DBA mice. Unlike Syrian hamsters, there does not appear to be a clear sex-related predisposition in most strains of mice, although it can be more common in males that are prone to fighting. The prevalence of spontaneous amyloidosis is significantly affected by stress, ectoparasitism, and chronic inflammatory conditions, such as ulcerative dermatitis, preputial adenitis, cervical lymphadenitis, conjunctivitis, and pyometra, among others. Individually housed SPF mice have a lower prevalence of amyloid compared to group housed mice. Localized forms of amyloidosis can also be found in mice. Tumor-associated amyloid can be found in pulmonary adenomas of A and BALB mice, and localized deposition in the corpora lutea is common in CBA and DBA mice, even though BALB and DBA mice are refractory to other forms of amyloidosis.
Amyloid has a characteristic hypocellular eosinophilic appearance in H & E-stained sections, and can be stained positively with Congo Red, Oil Red O, Alcian Blue, and Thioflavine T. Staining intensity may vary considerably. When stained with Congo Red and subjected to polarized light, amyloid is birefringent. Amyloid deposition occurs in renal glomeruli (Fig. 1.99), renal interstitium, lamina propria of the intestine (Fig. 1.100), myocardium, nasal submucosa, parotid salivary gland, thyroid gland, parathyroid gland, adrenal cortex, perifollicular areas of the spleen, pulmonary alveolar septa, periportal regions of the liver, tongue, testes, ovary, myometrium, aorta, pancreas, skin, and other tissues.
Intestinal deposition may be segmental in distribution.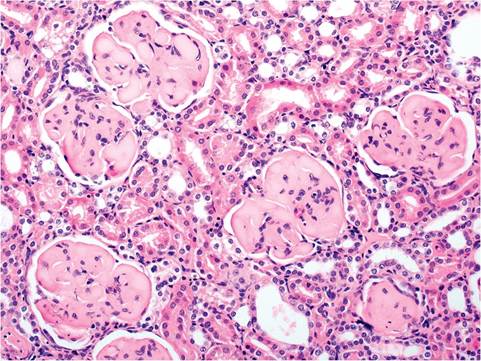
FIG. 1.99. Kidney from a mouse with renal amyloidosis, characterized by obliteration of the glomerular architecture by deposition of amyloid.
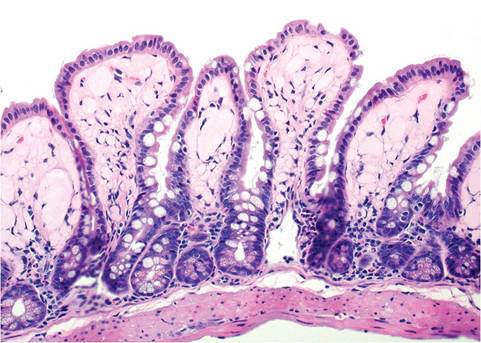
FIG. 1.100. Ileum from a mouse with intestinal amyloidosis. There is marked deposition of amorphous amyloid in the lamina propria.
Amyloidosis is often associated with cardiac atrial thrombosis with left- or right-sided congestive heart failure. The mechanism for this association is unknown but is probably related to renal disease. Mice with amyloid deposition in the renal medullary interstitium can develop papillary necrosis. Healed lesions give the illusion of hydronephrosis.
A common site of amyloid-like deposition is the nasal submucosa, particularly above the vomeronasal organs (Fig. 1.101). This material is not amyloid, as it does not stain with Congo Red, is Trichrome-positive, and PAS- positive after diastase treatment. Ultrastructurally, it consists of amorphous material and collagen. It is believed to be composed of complex carbohydrate that is secreted by nasal epithelium.
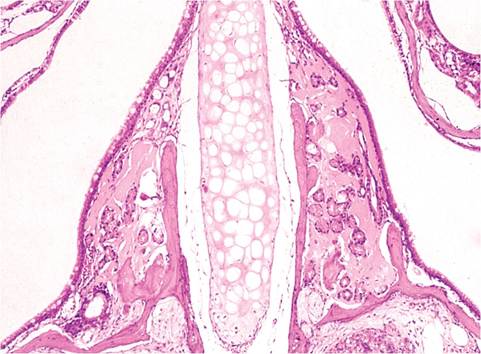
FIG. 1.101. Cross section through the nose of a mouse with deposition of amyloid-like material around submucosal glands. Although this material looks like amyloid in H&E stained sections, it is believed to be composed of complex carbohydrate originating from nasal glands.