Soft Tissue Calcification: Cardiac Calcinosis/ Myocardial Calcification
Spontaneous mineralization/calcification of the heart and other soft tissues is a common if not universal finding in BALB/c, C3H, and DBA mice. Lesions arise in mice as early as 3 weeks of age and increase with age.
Epicardial mineralization, accompanied by varying degrees of fibrosis, is found on the right ventricular free wall in BALB/c mice. In contrast, C3H mice do not develop epicardial mineralization, but rather develop foci of degeneration and mineralization throughout the myocardium of both ventricular walls and the interventricular septum. C3H mice also develop skeletal myofiber mineralization, particularly in axial muscles. DBA mice are especially prone to soft tissue mineralization. They develop both epicardial and myocardial mineralization, and dystrophic mineralization may also be found in aorta, testes, tongue, muscle, cornea, kidney, stomach, small intestine, and ovary. In the tongue, calcified nodules may form polypoid lesions. Dystrophic mineralization of the superficial corneal stroma is a common finding in DBA, C3H, and BALB (including C.B.-17-scid) mice. A variety of factors have been implicated in this condition, including environment, diet, concomitant disease, and elevated levels of corticosteroids. Female mice appear to be particularly at risk. The mineralization appears to be dystrophic in nature, since there is no evidence of elevated serum calcium levels in affected mice.There may be chalky linear streaks evident on the heart, particularly on the epicardium of the right ventricular free wall (Fig. 1.102). In young mice, these lesions are composed predominantly of mineral, but as mice age, they become enveloped in fibrous connective tissue

FIG. 1.102. Heart of a BALB/c mouse, depicting epicardial mineral deposition on the surface of the right ventricular free wall.
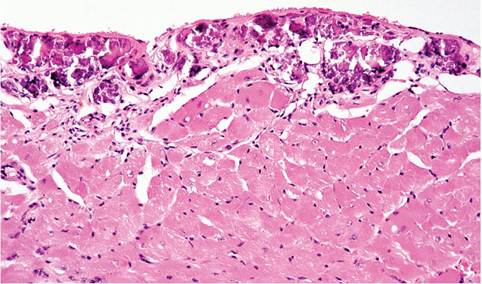
FIG. 1.103. Epicardial mineralization in a DBA mouse, illustrating deposition of mineral and fibrosis.
(Fig. 1.103). Myocardial lesions are present in the right and left ventricles, interventricular septum, and atria. Changes vary from single mineralized fibers to extensive linear calcification. In recent lesions, there may be interstitial edema. In lesions interpreted to be of some duration, there may be concurrent fibrosis and mononuclear cell infiltration. Foci of calcification in the tongue, when present, are often concentrated in the longitudinal musculature adjacent to the lamina propria, frequently with concurrent granulomatous inflammatory response and polyp formation. Lesions may be distributed anywhere along the tongue from the apex to the root of the tongue. Ulceration of the epithelium overlying affected areas is an infrequent finding. Foci of calcification, when present in the aorta, are characterized by mineralization of the elastic lamina and smooth muscle of the vessel wall. Corneal lesions are characterized by calcium deposition in the superficial layers of the corneal stroma. As lesions progress, deposits may become large aggregates of mineralized material, with stromal scarring, often leading to loss of overlying corneal epithelium and secondary ophthalmitis.