51 Palliative Care
Lauren Cobb T eresa P. Diaz-Montes
DEFINITIONS
Palliative Care
• Palliative care is specialized medical care for people with serious illnesses. The main focus is to provide patients with relief of distressing symptoms, pain, and the stress of a serious illness, irrespective of the prognosis.
Additionally, it focuses on the psychological and spiritual care as well as the development of a support system for the patient and their family and aims to improve their quality of life. The palliative care team is composed of physicians, nurses, and other specialists who work together with the patient's other physicians to provide an extra layer of support. It is appropriate at any age or at any stage in a serious illness and can be provided along with curative treatment. Benefits of palliative care are that it:• provides relief from pain, shortness of breath, nausea, and other distressing symptoms;
• affirms life and regards dying as a normal process;
• intends neither to hasten nor to postpone death;
• integrates the psychological and spiritual aspects of patient care;
• offers a support system to help patients live as actively as possible;
• offers a support system to help the family cope;
• uses a team approach to address the needs of patients and their families;
• enhances quality of life;
• is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy; and
• can be obtained in the hospital setting (inpatient palliative care unit or consult service), in the outpatient setting, or in hospice.
Hospice Care (End-of-Life Care)
• Hospice care is end-of-life care provided by health professionals and volunteers. The main goal is to provide medical, psychological, and spiritual support to the patient and their family.
Additionally, the primary focus is to assist the dying individual in achieving peace, comfort, and dignity during the process. The caregivers try to control pain and other symptoms so the individual can remain as alert and comfortable as possible. Usually, a hospice patient is expected to live 6 months or less. Hospice care can take place at home, at a hospice center, in a hospital, or in a skilled nursing facility. It serves to:• deliver palliative care to patients at the end-of-life and
• provide psychosocial care, nursing support, respite care, and bereavement support for the patient and their family.
• To obtain Medicare hospice benefits:
• Physician must certify that the patient has <6-month life expectancy assuming that the disease progresses as expected; there are no penalties for outliving the 6-month limit.
P.666
• Patient must qualify for Medicare Part A (insurance for hospital care and skilled nursing facility care).
• Patient selects a Medicare-approved hospice.
• Patient elects hospice care over regular Medicare care. However, Medicare will still cover regular medical expenses when not associated with the terminal illness.
• Physician Medicare benefits are maintained and patients can sign back on to Medicare whenever they wish.
• In general, comfort and quality of life are the primary goals. A “do not resuscitate” order is not necessary.
ETHICAL CONSIDERATIONS
Do Not Resuscitate/Do Not Intubate
• Do not resuscitate/do not intubate (DNR/DNI) is often a difficult discussion that patients expect their doctors to initiate. In general, the conversation should address the goals of treatment and the patient's priorities, including prolongation of life and quality of life, preferences for life-sustaining therapies, and goals for pain management.
• A patient can decide to be DNR/DNI but still pursue aggressive treatment; likewise, a patient can decide to pursue palliative treatment and still desire full resuscitation.
• Data show that resuscitation and intubation efforts in oncology patients are rarely successful.
• DNR/DNI discussion is urgently indicated if
• death is imminent or the patient is otherwise at high risk for intubation or resuscitation (e.g., compromised pulmonary function);
• the patient expresses a desire to die;
• the patient or her family wants to discuss hospice options;
• the patient has been recently hospitalized for progressing illness; or
• the patient has significant suffering coupled with a poor prognosis.
Legal Considerations
• The patient's decision may not always be the same as that of her physician or family.
• The principle of autonomy is an important consideration in American medicine.
• Living wills and DNR orders can ensure that patients' wishes are carried out.
• Situations in which patients' surrogate decision makers may disagree with previously formulated advance directives are common.
î Legally and ethically, a surrogate decision maker must clearly follow the advance directive formulated by a competent patient.
• Patients have the right to refuse or to withdraw care.
• Permitting death by not intervening is distinct from the action of killing.
• Physician-assisted suicide (i.e., a doctor provides a patient with the means to commit suicide with knowledge
of the patient's intent) is legal only in Oregon and Washington states.
• Voluntary euthanasia (i.e., an intervention to end a patient's life with her consent) is illegal in all states.
• Difficulties can arise when patients and their families request treatments considered futile or inappropriate by their physicians.
• No legal or societal consensus exists for situations in which patients and families disagree with physicians' recommendations to stop treatment.
P.667
• Consultation with an ethics committee or palliative care can be helpful.
• Excellent communication regarding educational, spiritual, and psychosocial needs can often resolve these conflicts.
END-OF-LIFE CARE: PAIN MANAGEMENT
• One of the most common and frightening symptoms for patients with terminal illness
• Patient surveys have shown that pain associated with advanced illness is often undertreated and that approximately 40% of cancer pain is undertreated.
• Pain should be addressed aggressively with multimodal therapy.
• The World Health Organization (WHO) pain ladder provides guidelines for pain control escalation (Fig. 511).
• Adjuvants include medicines, interventions, and alternative/complementary approaches designed to reduce fear or relieve anxiety.
• Pain can be visceral, somatic, or neuropathic; many patients have multifactorial pain.
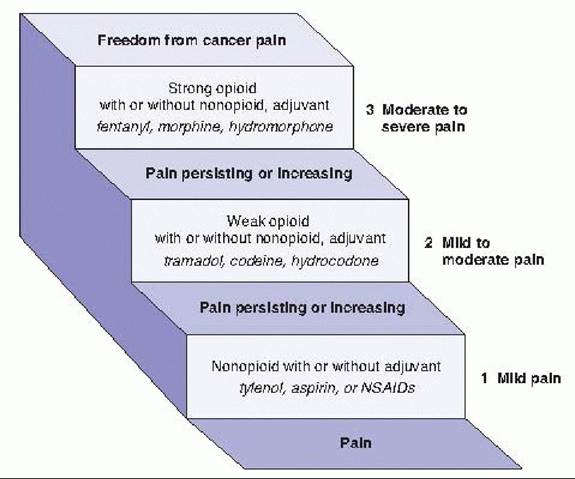
Figure 51-1. The WHO three-tier analgesia ladder depicts a rationale for escalating combination pain treatments as necessary to achieve pain control goals. Pain medications should be administered in order (nonopioids, then mild opioids like codeine, then strong opioids like morphine) until pain relief is achieved. Analgesics should be scheduled rather than given as needed. (Adapted from World Health Organization. Cancer pain relief and palliative care: report of a WHO expert committee. Geneva, Switzerland: World Health Organization, 1990:7-21.)
Medical T reatments
Nonsteroidal Anti-Inflammatory Drugs
• First step in the WHO pain treatment ladder
• Can act synergistically with opioids
P.668
• Should be given around the clock if pain is constant—twice daily options can aid in compliance
• No nonsteroidal anti-inflammatory drug (NSAID) has greater efficacy than another.
• Side effects include platelet inhibition (some nonsteroidals, such as Trilisate, do not inhibit platelets), gastrointestinal (GI) effects, and nephrotoxicity. These can be especially pronounced in older, frail patients.
• Often contraindicated in clinical trials or while receiving chemotherapy. GI prophylaxis is usually indicated for long-term palliative use.
• Acetaminophen is often just as effective and may be safer in some situations.
Opiates
• Second and third steps in the WHO ladder
• Opioids can be considered first line for terminal patients, especially those with severe pain.
• When pain is constant, escalate to around-the-clock dosing or longer acting narcotics with rescue doses as needed.
• There are various formulations and routes of administration (there is variation in response to these formulations and none are universally preferred over the other):
• Mu opioid receptors are a subset of opioid receptors that provide anesthesia in response to specific narcotics. Pure mu agonists specifically target these receptors for pain relief: morphine, fentanyl, oxycodone, hydromorphone, and methadone.
î Morphine: Available in oral tablets, solutions, elixirs, suppositories, and injectable formulas. Also available sublingually but is poorly absorbed in that route. Metabolized by the liver and excreted renally. Administer cautiously with renal insufficiency.
î Fentanyl: Available in transdermal, transmucosal, and injectable formulations. No active metabolites, which make it useful in renal insufficiency. Relatively lower propensity to cause histamine release and itching.
î Hydromorphone: Available in injectable and oral formulations and has a short half-life. Also useful in renal insufficiency, as its active metabolite is present in low concentration.
î Oxycodone: In formulations alone or mixed with acetaminophen. Available in immediate- or extended- release formulas.
o Methadone: Mu agonist but also W-methyl-D-aspartate antagonist which helps to reverse opioid tolerance. Long half-life. Risk of prolonging QT interval.
î Meperidine (Demerol) should be avoided, especially in renal failure, because its metabolite can accumulate and cause seizures.
î Partial agonist/antagonists (nalbuphine or buprenorphine) should be avoided because they can precipitate withdrawal.
î Refer to dosing guidelines (Table 51-1), as intravenous (IV) opioids are three times more potent than oral doses.
Hydromorphone and fentanyl are much more potent than other opiates.Severe Pain Crisis
• T reat with a rapid taper of a fast-acting IV narcotic or with IV patient-controlled analgesia (PCA).
• Once acute pain is controlled, calculate the dose and convert to a long-acting form.
Side Effects
• To alleviate side effects, decrease the dose, change to a different narcotic, change the route, or treat the symptoms.
P.669
• See the following text for treatment of nausea and vomiting.
• Constipation is frequently a problem for patients on around-the-clock opioid. A bowel regimen should be prescribed; senna is often the first choice.
• Sedation is common, although tolerance often develops.
• T reat pruritus with Benadryl or low-dose nalbuphine or naloxone.
TABLE 51-1 Opioid Analgesics: Equivalent Dosing for Various Narcotic Formulations
| Analgesic | Parenteral IM/IV Dose (mg) | Oral Dose (mg) | Half- lifea (hr) | Peak Effecta (hr) |
| Morphine | 10 | 30 | 2-3 | 0.5-1 |
| Hydromorphone | 1.5 | 7.5 | 2-3 | 0.5-1 |
| Meperidine | 75 | 300 | 2-3 | 0.5-1 |
| Fentanyl | 0.1 | Variable | 3-12 | 0.1 0.25 |
| Levorphanol | 2 | 4 | 12 15 | 0.5-1 |
| Oxycodone | NA | 20 | 2-3 | 1 |
| Codeine | 130 | 200 | 2-3 | 1.5-2 |
| Hydrocodone | NA | 30 | 4-6 | 0.5-1 |
| Methadone | 10 | 20 | 12- | 0.5-1.5 |
Use rows to convert dosing route and columns to convert between medications.
aParenteral dosing except for oral-only medications. IM, intramuscularly; IV, intravenous; NA, not available (oral only).
Adapted from Barakat RR, Markman M, Randall ME. Principles and Practice of Gynecologic Oncology. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:993.
Adjuvant Treatment
• Used to supplement or synergize with other pain medications
• Can be used to reduce narcotic dose and side effects
Neuropathic Pain
• Corticosteroids (such as dexamethasone) are often given as first line, especially with advanced cancer pain that exists with other symptoms.
• Tricyclic antidepressants are especially good for neuropathic pain.
• Side effects are related to their anticholinergic properties: sedation, urinary retention, dry mouth, constipation, dysphoria, and blurred vision.
• Can cause cardiac conduction abnormalities and decrease seizure threshold
• Other types of antidepressants (selective serotonin reuptake inhibitors [SSRIs]) also have some evidence for efficacy. They are particularly helpful in patients with both depression and neuropathic pain.
• Anticonvulsants can be used for neuropathic pain.
• Carbamazepine can be started at 100 mg orally (PO) twice a day (bid) and titrated up rapidly.
• Side effects include sedation, vertigo, hyponatremia, bone marrow suppression, and hepatotoxicity.
• Complete blood count and liver function tests should be followed.
P.670
• Phenytoin can be loaded as 20 mg/kg or 1,000 mg (whichever is less) IV and then 100 mg three times a day (tid).
• Side effects include anemia, anorexia, nausea/vomiting, hepatotoxicity, ataxia, bone marrow suppression, and hypersensitivity (fever, rash, hepatitis).
• GabapentinZpregabalin shows good efficacy in some randomized controlled trials for cancer.
• Must be started at low dose and titrated slowly.
• Principal side effect is sedation.
• All adjuvants for neuropathic pain generally take weeks for efficacy. Acute pain should be treated with acetaminophen, NSAIDs, and/or opioids.
• Capsaicin can be effective for neuropathic pain (especially zoster) but may burn when applied. Mechanism of action is depletion of substance P.
Bone Pain
• Bisphosphonates (osteoclast inhibitors) are useful to treat bone metastasis, breast pain, and possibly other cancers. They also prevent skeletal complications.
• Corticosteroids and NSAIDs can also be useful with pain from bone metastases.
Other Pain Symptoms
• Visceral crampy abdominal pain may be relieved by treating coexisting constipation or with anticholinergics such as hyoscyamine.
• Topical lidocaine—for sores or mucositis; lidocaine patch for herpes zoster.
Nonmedical and Invasive Treatments
• About 30% of cancer patients will have inadequate pain control despite large doses of opiates or will have intolerable side effects at opiate doses that do control pain.
• Radiation may be useful for bone metastasis and bulk effects.
• Chemotherapy may be useful for tumor effects, such as bowel obstruction.
• AnesthesiaZneurosurgical procedures
• Myofascial injections may work for pain from localized muscle contractions.
î Relief lasts from days to weeks.
• Neurostimulation (implanted device) has an unclear mechanism of action.
î Stimulation can be given to the spinal cord or thalamic nuclei.
î Spinal cord stimulators are electrodes placed in the epidural space. They are very expensive and require patient involvement which may not be ideal for end-of-life.
• Epidural or spinal PCA can decrease narcotic doses and reduce side effects.
• Somatic nerve block works for pain localized to a single nerve, plexus, or dermatome.
î A temporary injection is used to test for effectiveness.
î A neurolytic block can then be used for longer relief.
î The block can disrupt motor, sensory, or autonomic pathways.
• Sympathetic blocks can relieve visceral pain.
î Do not cause somatosensory or motor dysfunction
î A celiac plexus block can treat pain from the upper abdomen.
î Performed under fluoroscopic or computed tomography guidance.
î Almost all patients have transient hypotension, diarrhea, and back pain.
î Other complications include unilateral paresis and retroperitoneal bleeding.
î Superior hypogastric plexus blocks relieve pain from the pelvic viscera.
î Seventy-nine percent of patients achieve pain relief with a low complication rate.
P.671
• Surgery
• May be necessary for the most severe and persistent pain
• Vertebral body collapse and long bone fractures are treated best with prompt surgical intervention.
• Psychotherapy support groups, cancer counseling, and spiritual support
• Help patients deal with their diagnosis, decrease cognitive dissonance, and assist with coping skills
• Cognitive behavior techniques (progressive muscle relaxation, focused breathing, and meditation) require an alert patient but can be very helpful.
• T opical warm and cold treatments have few side effects.
• Can provide relief for muscle pain
• Transcutaneous electrical nerve stimulation and acupuncture
• No proven effect in randomized trials but virtually no side effects
END-OF-LIFE CARE: SYMPTOM MANAGEMENT
Respiratory Symptoms
Dyspnea
• Dyspnea is the sensation of uncomfortable breathing or shortness of breath.
• Differential diagnosis includes pulmonary embolus, pleural effusion, anemia, lung metastasis, pneumonia, anxiety, and fatigue/weakness.
• Treatment of the underlying cause (e.g., with antibiotics, anticoagulation, blood transfusion, thoracentesis) can provide relief.
• Oxygen and opiates can also relieve the sensation and reduce fear and anxiety.
• Increase opiates about 25% above baseline, just as for escalating pain treatment, for comfort.
• Benzodiazepines, corticosteroids, and bronchodilators may be useful.
Gastrointestinal Symptoms
Anorexia/Cachexia
• Usually a symptom of, not the cause of, functional decline. May be a symptom of the dying process.
• Anorexia refers to decreased appetite.
• Cachexia implies wasting; seen in cancer patients at the end-of-life.
• The pathophysiology of cachexia is not completely understood, but it appears to be related to decreased intake and increased cytokine levels.
• Cachexia does not respond well to nutritional supplements.
• Forced feeding often produces no weight gain and can increase patient discomfort and nausea.
• Treatment
• Appetite stimulants can restore appetite briefly but have multiple side effects and are not associated with improved survival.
î Use when appetite is a significant quality of life issue and potential benefits outweigh side effects.
• Only two classes of drugs are well supported by multiple randomized trials:
î Dexamethasone 4 mg daily; side effects are those associated with chronic steroid use.
î Megace 400 to 800 mg daily; liquid and long-lasting forms are available. Significant side effects.
P.672
• Artificial nutrition is indicated only for patients who are unable to eat (e.g., bowel obstruction) and have relatively good prognosis (3 months or greater). Substantial adverse effects.
Nausea/Vomiting
• May result from chemotherapy, opiates, or disease progression.
• The type of nausea may determine treatment strategy:
• Acute (within 24 hours of a treatment or procedure)
• Delayed (after 24 hours)
• Anticipatory (a conditioned response after severe nausea and vomiting in the past)
• Treatment: Around-the-clock dosing with rescue and escalation regimens using drugs from different categories is often successful. Multiple receptor-signaling pathways in the area postrema have been suggested to mediate nausea and vomiting.
• Anticholinergic drugs act mainly on muscarinic receptors.
î Scopolamine 1.5 mg transdermally q72hr
î Side effects include dry mouth, drowsiness, and visual changes.
• Antihistamines have sedation as their greatest side effect.
î Diphenhydramine (Benadryl) 25 to 50 mg PO q6hr or 10 to 50 mg IV
î Dimenhydrinate (Dramamine) 50 mg PO q4hr
î Cyclizine (Marezine) 50 mg PO/intramuscularly (IM) q4hr or 100 mg per rectum (PR) q4hr
î Meclizine (Antivert) 25 to 50 mg PO daily (qd)
î Promethazine (Phenergan) 12.5 to 25 mg PO/IM q4hr or PR q12hr
• Dopamine receptor antagonists
î Phenothiazines may lead to extrapyramidal reactions which can be treated with diphenhydramine.
î Prochlorperazine (Compazine) 5 to 10 mg PO q6hr or 2.5 to 10 IM/IV q3hr or 25 mg PR q12hr
î Chlorpromazine (Thorazine)
î Haloperidol (Haldol)
î Side effects include akathisia, dystonia, and tardive dyskinesia.
î Metoclopramide (5 to 10 mg PO/IV/IM q6hr) is a modest antiemetic and increases gastric emptying.
• Serotonin antagonists are highly efficacious but very expensive. Side effects are mild, including headache and constipation. Granisetron, dolasetron, and palonosetron are in this category and have equivalent efficacy.
• Neurokinin receptor antagonists are a newer option.
î Aprepitant is approved for short-term use only, with highly emetogenic chemotherapy.
• Other antiemetics have unclear mechanisms of action.
î Corticosteroids are especially effective for chemotherapy-induced nausea.
î Cannabinoids have modest antiemetic effects.
î Dronabinol 5 to 10 mg PO q6hr is the legal prescribable form.
î Benzodiazepines are weak antiemetics but are very good at treating anxiety, which can contribute to nausea.
î Small studies have shown that acupuncture has some antiemetic effects.
• Prophylaxis
• The appropriate method depends on the emetogenic property of the chemotherapy.
• If severe nausea has occurred with a particular regimen, treatment should be escalated.
P.673
• Agents with very low emetogenic risk usually require no prophylaxis.
• Low-risk regimens: dexamethasone 20 mg IV or prochlorperazine 10 mg PO once before chemotherapy
• Moderate- to high-risk regimens: serotonin antagonist, such as ondansetron (oral dosing equivalent to IV) plus dexamethasone 8 mg IV prior to chemo, followed by dexamethasone 4 to 8 mg PO bid ? 2 more days to prevent delayed nausea
• Extremely high-risk chemotherapy (especially cisplatin): serotonin antagonist plus dexamethasone 8 mg IV plus aprepitant 125 mg PO prior to chemo, followed by dexamethasone 8 mg PO qd ? 3 days and aprepitant 80 mg PO qd ? 2 days.
• Anticipatory nausea can be treated with alprazolam 0.5 to 2 mg as needed.
Ascites
• A frequent problem in late-stage ovarian cancer
• Not many treatment options are available.
• High-dose spironolactone has shown some benefit in small trials.
• Therapeutic large-volume paracentesis can be performed for acute relief:
î Mean duration of relief is only 10 days.
î Large-volume drainage leads to hypovolemia.
î Repetitive taps increase the risk of infection.
î If more than 5 L are drained, albumin can be given.
• Permanent catheters (PleurX) are available and may reduce infection risk; patients can drain ascites at home.
Bowel Obstruction
• Bowel obstruction is frequent in ovarian cancer patients.
• Small bowel obstruction (SBO)
• Usually managed conservatively with bowel rest and decompression (i.e., nasogastric tube) unless bowel ischemia or strangulation is present.
• Further intervention depends on the clinical situation.
î Surgery should not occur routinely in patients with very poor prognosis (e.g., massive ascites, multiple sites of obstruction, diffuse carcinomatosis, or poor performance status).
î Obstruction can be relieved by surgery, but perioperative morbidity and mortality are high. Reobstruction is common.
• A percutaneous gastrostomy tube can be placed for venting.
• Hyoscyamine or octreotide (0.3 to 0.6 mg subcutaneous [SQ]) decreases gastric secretion and slows intestinal motility, thereby decreasing the nausea/vomiting associated with SBO. This is supported by several randomized trials.
• Colonic obstruction
• Less frequent than SBO
• Surgical correction is indicated.
• Endoscopic stents may work for palliative treatment.
• Acute colonic pseudo-obstruction
• Mimics anatomic obstruction which must be ruled out by imaging.
• Follow with serial abdominal exams and daily x-rays.
• Supportive care with bowel rest is often enough to reverse the pseudo-obstruction.
• Low magnesium, calcium, and potassium should be replaced.
• Neostigmine 2 mg IV ? 1 can be used; however, some patients experience bradycardia and should be monitored in an intensive care setting with atropine available.
P.674
• Endoscopic decompression with placement of a rectal tube may be attempted if neostigmine fails, if evidence of decompensation exists, or if the bowel diameter is >13 cm.
• Surgery should be attempted if the aforementioned measures fail.
Constipation
• Constipation is common for patients on opiates. Both prophylaxis and treatment are indicated.
• T reatment regimens should incorporate multiple mechanisms of action.
• Fiber and bulk-forming laxatives are usually contraindicated for palliative care.
• Hyperosmolar laxatives draw water into the stool (polyethylene glycol 240 to 720 mL a day; lactulose 15 to 30 mL bid; sorbitol 120 mL of 25% solution daily; and glycerine 3 g PR daily or 5 to 15 mL enemas).
• Saline laxatives are also hyperosmolar (magnesium sulfate 15 g daily, magnesium citrate 200 mL daily).
• Stool softeners are usually ineffective when used alone (docusate sodium 100 mg PO bid, mineral oil 15 to 45 mL a day).
• Stimulants increase bowel motility (Bisacodyl 30 mg PO qd or 10 mg PR qd and senna 1 to 4 tsp qd).
• Fecal impaction should be treated aggressively.
• Can be extremely painful and even lead to mental status changes
• Mechanical disimpaction is required, followed by enemas. Colonic cleanout with polyethylene glycol is important, and aggressive bowel therapy should be started to prevent a recurrence.
Constitutional Symptoms
Fatigue
• The pathophysiology of fatigue from cancer is unclear.
• Can significantly decrease quality of life
• Differential diagnosis includes anemia, chronic stress reaction, inflammation/immune reaction, disrupted circadian rhythm or sleep disturbance, hormonal changes, depression, and direct central nervous system toxicity.
• Evaluation of reversible causes should be initiated.
• Workup includes evaluation of disease progression, medication effects and interactions, hematocrit, electrolytes, pain assessment, depression risk, and medical comorbidities.
• At the end-of-life, reassurance for the family may be the most appropriate step.
• Treatments:
• Severe anemia may be treated with red cell transfusion, erythropoietin injection, iron, folic acid, and vitamin B12 supplementation.
• Moderate exercise may reduce fatigue and improve functional status in healthier patients. Energy conservation (including limiting/scheduling activities) is more appropriate in patients with more advanced illness.
• Sleep hygiene and cognitive behavioral therapy can increase the effectiveness of sleep.
• Psychostimulant use is not well supported (methylphenidate 5 mg PO every morning and noon to start; modafinil, a nonamphetamine activating agent, 100 to 200 mg every morning and at noon can be used in some situations).
• Antidepressants may decrease fatigue associated with depression. Nortriptyline has sedative properties but can be useful for insomnia and poor sleep hygiene contributing to fatigue; alternatively, bupropion is more activating.
P.675
Neurologic Symptoms
Insomnia
• Often alleviated by treating underlying pain, anxiety, depression, or by addressing psychosocial/spiritual issues. Consider delirium in the diagnosis.
• When initial treatment is ineffective, a hypnotic agent can be used short term.
• In patients already on hypnotics, reduced dosing may restore normal sleep patterns.
• Sleep hygiene is often helpful.
Delirium/Agitation
• Mental status changes can be very distressing for families and can complicate home care.
• Workup depends on the patient's status and preferences.
• The mnemonic DELIRIUM can be helpful:
D: drugs (e.g., anticholinergics, ranitidine, lorazepam, opiates)
E: electrolytes, emotions (e.g., hyponatremia, hypophosphatemia, hyperammonemia)
L: low O2, lack of drugs (e.g., pneumonia, pulmonary embolus, withdrawal)
I: ictal (e.g., stroke, brain metastases, seizure disorder)
R: retention (e.g., of CO2, urine, or stool)
I: ischemia, infection (e.g., transient ischemic attack, stroke, meningitis, urosepsis, pneumonia)
U: uremia (e.g., renal failure)
M: myocardial (e.g., infarction, arrhythmia, heart failure)
• Rapid sedation with haloperidol 0.5 to 1 mg IV/PO/SQ, repeated as needed and coupled with lorazepam 0.5 to 1 mg PO/IV q1 to 2hr may be helpful.
Symptoms from Distant Metastases
Bone Metastases
• Can be very painful and lead to pathologic fractures
• Localized radiation provides pain relief in 35% to 100% of patients but has toxicity including mucositis, enteritis, dermatitis, and bone marrow suppression.
• Can often be relieved with single treatment (well supported by randomized trials) but may take several weeks for full efficacy
• Hemibody radiation can be used for diffuse metastasis but has complications including radiation pneumonitis.
• Surgical fixation is appropriate for fractures and some impending fractures.
• Bisphosphonates decrease the rate of skeletal complications in breast cancer, but their role in the treatment of bone pain and in other cancers is less clear.
• Consider NSAIDs and steroids.
• Calcitonin has not been shown to relieve bone pain from metastasis.
Brain Metastases
• Initial presentation may be seizures, nausea/vomiting, persistent headache, neurologic symptoms, or cognitive/personality changes.
• Magnetic resonance imaging (MRI) is usually necessary for diagnosis.
• Symptomatic patients receive dexamethasone 10 mg then 4 mg PO every 6 hours.
• Response is usually within 24 to 72 hours.
• Patients are at risk for opportunistic infections. Pneumocystis carinii pneumonia prophylaxis should be initiated.
• Proton pump inhibitor prophylaxis is appropriate.
P.676
• Wean steroids to lowest effective dose.
• Prophylactic seizure medication is not required, but treatment is necessary if seizures persist.
• Radiation can reduce symptoms and improve survival, depending on patient prognosis.
Spinal Metastases
• Cause bone pain, cord compression, fractures, leptomeningeal metastasis, and malignant plexopathy
• Epidural spinal cord compression requires rapid diagnosis and treatment to avoid permanent paralysis.
• Presentation is pain progressing to weakness and hyperreflexia, followed by bowel and bladder dysfunction and paralysis.
• An MRI should be obtained on all cancer patients with new or worsening back pain.
• Treatment:
• Steroids relieve pain and decrease the rate of neurologic complications.
î Low-dose regimen: 10 mg load then 16 mg a day tapered over 2 weeks.
î High-dose regimen: 100 mg IV load then 24 mg tid for 3 days, tapered over 10 days. There are significant side effects with this dosing regimen.
• Spinal cord compression requires urgent radiation treatment or surgical decompression.
• Radiation treats pain and stabilizes neurologic function.
• Eighty percent to 100% of patients who are walking at the time of radiation will retain function; patients who have lost function are unlikely to regain it.
Other Considerations
Hydration
• The decision to begin or continue hydration can be difficult at the end-of-life; treatment should be formulated in consultation with the patient and her family.
• There is no evidence that hydration improves patient comfort.
• Dry mouth is best treated with mouth swabs.
• May prolong death process and increase secretions and edema. IV access may be difficult.
• May decrease electrolyte-induced delirium
Palliative Sedation
• Rarely used except for extreme symptom control
• Use of benzodiazepines or phenobarbital at end-of-life should be discussed.
• Palliative care consultation may be helpful before initiating heavy sedation.
Death Rattle
• The course rasps at the end-of-life are sometimes described as a “death rattle.”
• A scopolamine patch can help decrease these distressing sounds.
Depression
• Adjustment reaction to a terminal diagnosis is expected; however, depression should be formally evaluated and treated when diagnosed.
• Counseling and cognitive behavioral therapy are useful adjuncts.
• All antidepressants have side effects, which should be considered in the choice of treatment.
• Tricyclic antidepressants are sedating and have anticholinergic effects (e.g., dry mouth, constipation, urinary retention).
• SSRIs are less sedating and less anticholinergic than tricyclics.
• Bupropion can lower seizure threshold.
P.677
Anxiety
• Benzodiazepines are the mainstay of acute treatment.
• Short acting: alprazolam 0.25 to 1 mg PO tid or four times a day; lorazepam 0.5 to 2 mg PO/IV/IM q3 to 6hr
• Longer acting: clonazepam 1 to 2 mg PO bid; diazepam 2.5 to 10 mg PO/IV/IM q3 to 6hr
• Many antidepressants, especially SSRIs, also have anxiolytic effects.
• Neuroleptics may be used if benzodiazepines are ineffective: thioridazine 10 to 25 mg PO tid; haloperidol 0.5 to 5 mg PO/IV/SQ q2 to 12hr
• Other options include methotrimeprazine 10 to 20 mg IM/IV/SQ q4 to 8hr and chlorpromazine 12.5 to 50 mg PO/IM/IV q4 to 12hr. These are more sedating but are also analgesic.
• Atypical antipsychotics:
• Olanzapine 2.5 to 10 PO qd and risperidone 0.5 to 4 PO qd may be useful in frail, older patients.
• Buspirone 10 PO tid may be used for chronic anxiety; takes 5 to 10 days to see any effect.
Spiritual/Existential Issues
• Concerns about maintaining personal dignity, lack of closure in relationships, inability to discern meaning in life, and spiritual crisis are often very distressing to patients.
• Counseling and early involvement of a spiritual counselor can often give comfort.
SUGGESTED READINGS
Chase DM, Monk BJ, Wenzel LB, et al. Supportive care for women with gynecologic cancers. Expert Rev Anticancer Ther 2008;8(2):227-241.
Doyle D, Woodruff R. The IAHPC Manual of Palliative Care, 2nd ed. Houston, TX: International Association
of Hospice and Palliative Care, 2004.
Grant M, Elk R, Ferrell B, et al. Current status of palliative care clinical implementation, education, and research. Cancer J Clin 2009;59:327-335.
Sepulveda C, Marlin A, Yoshida T, et al. Palliative care: the World Health Organization’s global perspective. J Pain and Symptom Manage 2002;24(2):91-96.
2A 2 g dose is recommended in women with a BMI ≥35 or weight greater than 100 kg or 220 lbs.
Moderate or severe uncontrolled HTN
History of CVA or MI
Multiple risk factors for CAD: age, smoking, HTN, DM
History of or current DVT/PE
Migraines with aura or focal neurologic symptoms
Active hepatoma or liver cirrhosis or unexplained elevation of liver enzymes
Known or suspected breast cancer
Smoking >15 cigarettes per day and age >35 yr
Breast-feeding <6 wk postpartum (theoretic risk of growth restriction)
Diabetic neuropathy, retinopathy, neuropathy, or other vascular disease
Valvular heart disease, complicated (SBE, pulmonary HTN, or atrial fibrillation)
Known thrombogenic mutation
aNot studied in CREST.
Data from Peterson HB, Xia Z, Hughes JM, et al. The risk of pregnancy after tubal sterilization: findings from the U.S. Collaborative Review of Sterilization. U.S. Collaborative Review of Sterilization Working Group. Am J Obstet Gynecol 1996;174:1161-1170; Kovacs GT, Krins AJ. Female sterilizations with Filshie clips: what is the risk failure? A retrospective survey of 30,000 applications. J Fam Plan Reprod Health Care 2002:28:34-35.
Hysteroscopic Tubal Sterilization (Essure Micro-Insert)
• Essure is an irreversible method of transcervical hysteroscopic tubal occlusion that can be performed in the