50 Chemotherapy and Radiation Therapy
Sonia Dutta
Amanda Nickles Fader
• T reatment of gynecologic cancer typically requires a multidisciplinary and multitreatment approach involving a combination of surgery, chemotherapy, and radiation therapy.
When more than one modality is used, they may be delivered sequentially or at the same time, as with chemoradiation or intraoperative radiation therapy. The sequence of treatment is characterized as “primary,” referring to initial treatment; “adjuvant,” referring to secondary treatment for micrometastatic disease after surgical management; “neoadjuvant,” referring to induction chemotherapy, radiation therapy, or both administered before definitive therapy; and “salvage,” referring to treatment at time of recurrence.All methods used to treat gynecologic cancer can cause damage to normal tissue. Therefore, the governing principle of both chemotherapy and radiation therapy is to attain maximal therapeutic cytotoxic effects on cancer cells without extreme toxicity to normal tissues. Unfortunately, it is not always possible to obtain a therapeutic effect without temporarily or permanently altering the functions of other healthy cells, tissues, or organs. The term therapeutic index is the ratio of a toxic dose to the curative dose. An optimal treatment goal is to use chemotherapy agents and radiation doses that have a high therapeutic index.
CELL CYCLE
• T umor cells grow as a result of deregulation between proliferation and suppression. Our understanding of cancer cell kinetics and the classical cell cycle (Fig. 50-1) has led to the development of several chemotherapy drugs. There are both cell cycle-specific chemotherapeutic agents and cell cycle-nonspecific chemotherapeutic agents.
• Cell cycle-specific agents depend on the proliferative capacity of the cell and the phase of the cell cycle for their action. They are effective against tumors with relatively long S phases and rapid proliferation rates.
• Cell cycle-nonspecific drugs kill cells in all phases of the cell cycle and their effectiveness is not dependent on proliferative capacity. Radiation therapy is not cell cycle dependent.
CHEMOTHERAPY
Types of Chemotherapy
• Chemotherapeutic agents commonly used for the treatment of gynecologic cancer may be grouped into the following categories (Table 50-1):
• Alkylating agents are cell cycle-nonspecific. They contain an alkyl group that forms a covalent bond with the DNA helix, preventing DNA duplication. They
P.654 also function by attaching to free guanine bases of DNA thereby prohibiting their action as templates for new DNA formation.
• Antimetabolites are similar in chemical structure to compounds required by normal and tumor cells for cell division. These antimetabolites may be incorporated into new nuclear material or combined with enzymes to inhibit cell division.
• Plant alkaloids are derived from various plants and trees, including the periwinkle plant (Vinca rosea), the mayapple (Podophyllum peltatum), and the Pacific yew (Taxus brevifolia). They bind to tubules, blocking microtubule formation, and interfering with spindle formation. This leads to the arrest of metaphase and inhibits mitosis.
• Antitumor antibiotics have many different modes of action, including increasing cell membrane permeability, inhibiting DNA and RNA syntheses, and blocking DNA replication.
• Biologics target known mutations to oncogenic signal transduction pathways specific to cancer cells. As cancer biology is further elucidated, increasing numbers of biologics are being discovered and tested.
• Miscellaneous agents have different modes of action than those previously mentioned.
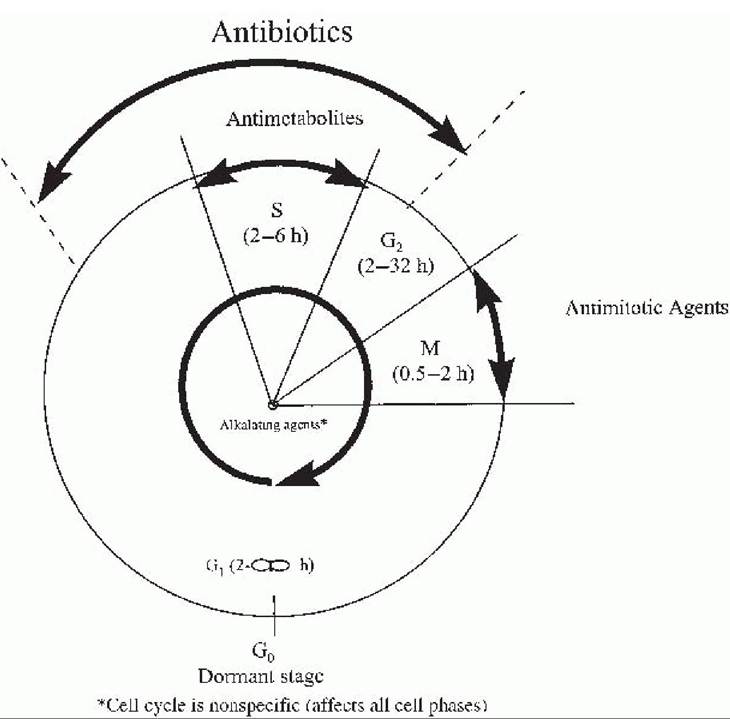
Figure 50-1. Phases of the cell cycle, relative time intervals, and sites of action of the various classes of antineoplastic agents. (From Trimble EL, Trimble CL, eds. Cancer Obstetrics and Gynecology.
Philadelphia, PA Lippincott Williams & Wilkins, 1999:60, with permission.)
TABLE 50-1 Chemotherapeutic Agents Frequently Used in Gynecologic Cancer and Their Most Common Toxicities

Alkylating agents
| Cyclophosphamide (Cytoxan) | Myelosuppression (WBCs > platelets), hemorrhagic cystitis, bladder fibrosis, alopecia, hepatitis, amenorrhea |
| Ifosfamide | Myelosuppression, hemorrhagic cystitis, CNS dysfunction, renal toxicity, emetogenic |
Alkylating-Iike agents
| Cis- dichlorodiaminoplatinum (Cisplatin) | Nephrotoxicity, emetogenic, tinnitus and hearing loss, myelosuppression, peripheral neuropathy characterized by paresthesia of the extremities |
| Carboplatin | • Renal insufficiency is the major dose-limiting toxic effect causing elevations in BUN, serum creatinine, and serum uric acid levels within 2 wk of treatment. Irreversible damage can occur. Prevention with IV hydration and diuretics is important during treatment. A 24-hr creatinine clearance is measured to establish baseline renal function before treatment. • Tinnitus or high-frequency hearing loss may be cumulative and possibly irreversible. Audiograms may be obtained before and during treatment to assess hearing loss. Less neuropathy, ototoxicity, and nephrotoxicity but more myelosuppression (platelets > WBC) than cisplatin |
Antitumor antibiotics
| Actinomycin D (Dactinomycin) | Nausea and vomiting, skin necrosis, mucosal ulceration, myelosuppression, alopecia |
| Bleomycin sulfate | Pulmonary toxicity, fever, anaphylactic reactions, dermatologic reactions, mucositis, alopecia • May cause significant pulmonary fibrosis. Generally, both dose- and age-related but can be idiopathic. Pulmonary function tests are performed to assess baseline pulmonary capacity before the first dose is administered.• Can cause anaphylaxis, skin reactions, fever, and chills. Because of the high incidence of allergic reactions, patients are given a test dose of 2-4 U intramuscularly before the first dose of drug. |
| Doxorubicin hydrochloride (Adriamycin) | Myelosuppression, cardiac toxicity, alopecia, mucosal ulcerations, emetogenic, cholestasis, hyperpigmentation |
| Irreversible cardiomyopathies that involve progressive congestive heart failure, pleural effusions, heart dilation, and venous congestion. These are generally cumulative; therefore, dosages are kept under the maximum. Multiple-gated acquisition (MUGA) scans are commonly obtained before treatment to obtain a baseline ejection fraction and may be repeated as necessary. | |
| Liposomal doxorubicin (Doxil) | Myelosuppression, skin and mucosal toxicity, hand-foot syndrome |
Antimetabolites
| 5-Fluorouracil (5-FU) | Myelosuppression, emetogenic, anorexia, alopecia, hyperpigmentation, mucosal ulceration, cardiotoxic (MI, angina, arrhythmia) |
| Methotrexate sodium (MTX) | Myelosuppression, mucosal ulceration (stomatitis and mucositis), hepatotoxicity, acute pulmonary infiltrates that respond to steroid therapy, emetogenic, alopecia, peripheral neuropathy |
| Gemcitabine hydrochloride (Gemzar) | Mild myelosuppression, flu-like syndrome, emetogenic |
Plant alkaloids
| Vincristine sulfate (Oncovin) | Neurotoxicity (peripheral, central, and visceral neuropathies that are cumulative), alopecia, myelosuppression, cranial nerve palsies |
| Epipodophyllotoxin (etoposide, VP-16) | Myelosuppression, alopecia, hypotension, allergic reaction, emetogenic |
| Paclitaxel (Taxol) | Myelosuppression (WBC > platelets), alopecia, allergic reactions, cardiac arrhythmias, peripheral neuropathies, emetogenic • Asymptomatic and transient bradycardia (40-60 beats/min), ventricular tachycardia, and atypical chest pain during infusion. These symptoms resolve with slowing of infusion.• Hypersensitivity reactions with characteristic bradycardia, diaphoresis, hypotension, cutaneous flushing, and abdominal pain. Premedications of diphenhydramine hydrochloride, dexamethasone, and ranitidine are given prophylactically. |
| Docetaxel (Taxotere) | Myelosuppression (neutropenia), hypersensitivity; cutaneous reactions, alopecia, mucosal ulcerations, paresthesias |
Biologics
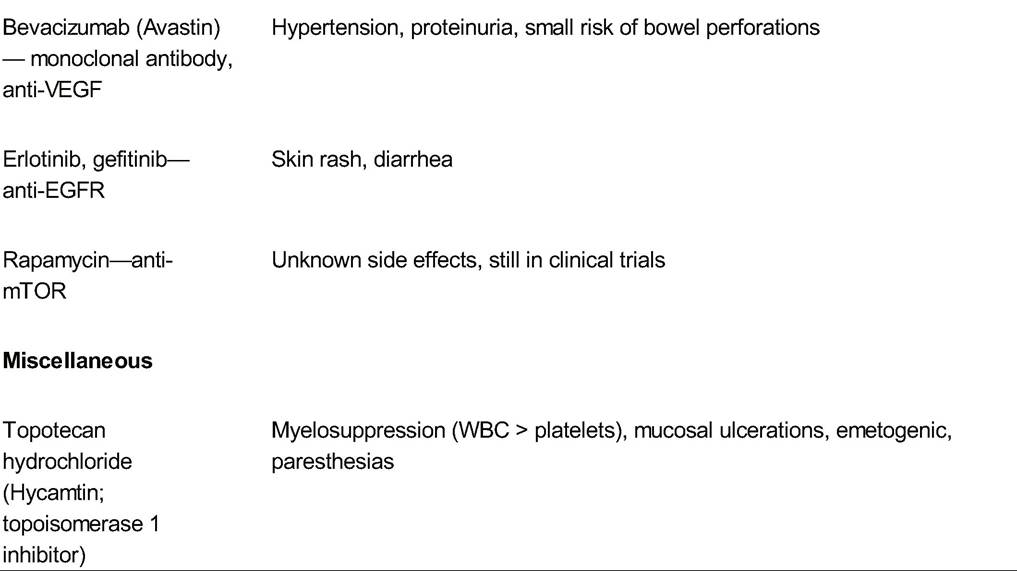
WBC, white blood cell; CNS, central nervous system; BUN, blood urea nitrogen; IV, intravenous; MI, myocardial infarction; VEGF, vascular endothelial growth factor; EGFR, epidermal growth factor receptor; mTOR, mammalian target of rapamycin.
Common Side Effects of Chemotherapy
• Hematologic toxicity and myelosuppression is a dangerous effect of chemotherapy that varies in severity depending on the drug administered. A nadir in white cell, red cell, or platelet count is usually observed 7 to 14 days after drug administration. Most agents are readministered every 3 to 4 weeks if the patient has recovered from pancytopenia.
• Neutropenia is defined as an absolute neutrophil count (ANC) less than 500/mL. Recombinant human granulocyte colony-stimulating factor (G-CSF) (filgrastim, Neupogen) or pegylated filgrastim (Neulasta) is administered to at-risk patients or the cycle after neutropenia is diagnosed as prophylaxis against this reaction in subsequent cycles. Use of G-CSF is contraindicated during the actual administration of chemotherapy or during a neutropenic fever.
• Neutropenic fever is a medical emergency, as these patients can quickly become septic and decompensate. Common causes of infection include enteric Gramnegative bacteria, Gram-positive bacteria (Staphylococcus epidermidis, Staphylococcus aureus, and diphtheroids), viruses (herpes simplex and herpes zoster), and
P.658 fungi (Candida and Aspergillus species), although often an offending agent is not identified.
Infections are generally due to reduced integrity of the mucous membranes and skin during chemotherapy. Once fever (temperature greater than 38°C) is noted, broad-spectrum antibiotics with antipseudomonal coverage should be initiated immediately.• Anemia can be treated acutely with blood transfusions. Long-term treatment may be accomplished with ferrous sulfate and erythropoietin-stimulating agents (e.g., epoetin α, Epogen, Procrit). The target is a hemoglobin level of 10 g/dL or hematocrit of 30%, although all of these interventions have potentially
significant risks that must be considered against their benefits prior to their use.
• Thrombocytopenia is treated with platelet transfusion when the platelet count drops below 20,000/mL or if signs of spontaneous bleeding are evident. Thrombopoietin (e.g., oprelvekin [Neumega]) may also be given.
• Gastrointestinal toxicity is commonly seen due to the direct action of chemotherapy on these cell types.
• Nausea and vomiting are the most common side effects of chemotherapy due to decreased intestinal motility. The severity and incidence of these symptoms vary greatly but the inability to effectively control them can result in patient refusal to carry out potentially curative treatment. Nausea and vomiting can be
î acute—occurring during or immediately after chemotherapy administration,
î delayed—occurring several days after chemotherapy administration, and
î anticipatory—occurring before the administration of chemotherapy.
• The incidence and severity are related to the emetogenic potential of the drug, the dose, the route and time of day of administration, patient characteristics, and the combination of drugs used. Gastrointestinal obstruction must be considered if abdominal distention or obstipation is present.
• Antiemetic regimens including a combination of serotonin 5-HT3 receptorblocking agents (e.g., ondansetron, granisetron), neurokinin receptor antagonists (e.g., aprepitant, fosaprepitant), and dexamethasone have been shown to be particularly effective in reducing acute and delayed emesis.
• Diarrhea may occur in association with chemotherapy and is typically not infectious; however, necrotizing enterocolitis must always be considered if diarrhea is watery, bloody, and associated with abdominal pain and fever.
• Stomatitis and mucositis occur most commonly following therapy with antimetabolites because these cells are naturally rapidly proliferating. Treatment is with either Larry's solution (three equal parts diphenhydramine hydrochloride elixir [Benadryl], magnesium and aluminum oral suspension [Maalox], and viscous lidocaine) or nystatin swish and swallow. Severe cases may require hospitalization for nutrition supplementation, intravenous (IV) hydration, and pain management.
• Dehydration may occur in the setting of emesis and diarrhea. Patients are encouraged to increase their fluid intake to prevent postchemotherapy dehydration, given the risk of secondary side effects, such as nephrotoxicity or electrolyte disturbances.
• Hepatic toxicity including transient elevations in transaminase and alkaline phosphatase levels may occur with chemotherapy. Cholangitis, hepatic necrosis, and hepatic veno-occlusive disease, although rare, must be considered.
• Common dermatologic toxicities are alopecia and photosensitivity. Extravasation of chemotherapeutic agents can additionally cause skin necrosis. Once identified, the infusion should be immediately stopped and the patient given topical steroids and hyaluronidase or sodium thiosulfate.
P.659
• Acute allergic or infusion reactions may occur with the use of chemotherapeutic agents. For agents that cause hypersensitivity, such as paclitaxel, premedication with diphenhydramine hydrochloride, dexamethasone, and ranitidine are given. For agents that may cause anaphylaxis, such as bleomycin, a test dose should be performed prior to administration. Platinums are notorious for causing an allergy after several doses of the medication has been administered, and prompt recognition of anaphylaxis is key.
• Neurologic side effects of chemotherapy include damage to peripheral nerves as well as subtle changes in cognitive function. Peripheral nerve damage may range from transient paresthesias, such as a “pins-and- needles” sensation, to chronic loss of sensitivity and fine motor control. Changes in cognitive function are generally perceived as difficulties with concentration and short-term memory. To date, there are no interventions proven to prevent or ameliorate this neurologic damage.
• Fatigue is commonly reported. The mechanisms causing fatigue are not well understood; however, correction of anemia, good sleep hygiene, and regular exercise can help reduce symptoms.
• Pulmonary toxicity in the form of interstitial pneumonitis with pulmonary fibrosis is classically seen with bleomycin. Once diagnosed, the medication should be stopped and steroids started.
• Cardiac toxicity is rare with chemotherapy because myocytes do not readily divide. However, doxorubicin is classically associated with cardiomyopathy. Additionally, use of bevacizumab (Avastin) has been associated with the development of hypertension.
• Genitourinary toxicity is typically seen in the form of renal tubular toxicity with platinums, especially cisplatin.
• Additionally, hemorrhagic cystitis can occur with ifosfamide and cyclophosphamide treatment. Preventive measures include hydration and administration of diuretics. Treatment includes dosage reduction or discontinuation of the drug. Mesna, a uroprotector, is administered simultaneously with ifosfamide to protect against bladder toxicity. Mesna acts to detoxify acrolein, the common metabolite of both cyclophosphamide and ifosfamide.
RADIATION THERAPY
• X-rays or gamma rays destroy tumor and normal cells by creation of oxygen-free radicals and a multitude of other reactions ultimately resulting in DNA and cell membrane injury.
• The absorption of energy by tissue is measured in rads. One gray (Gy) is 100 rad and 1 centigray (cGy) is 1 rad. The inverse square law states that the dose of radiation at a given point is inversely proportional to the square of the distance from the source of radiation.
Clinical Radiation Sources
• Teletherapy is external beam radiation. During external beam radiation, the patient may be in prone or supine position. The usual total dose to the pelvis ranges from 4,000 to 5,000 cGy given in daily fractions of 180 to 200 cGy over 5 weeks.
• Brachytherapy involves placement of a radiation device either within or close to the target tumor volume (i.e., interstitial and intracavitary irradiation); the radiation dose to the tissue is determined largely by the inverse square law.
P.660
• The radiation applicators are called intrauterine tandems and ovoids/colpostats. Intrauterine tandems are placed in the uterine cavity while the patient is under anesthesia and position is confirmed with radiographic studies. Vaginal ovoids are designed for placement in the vaginal vault and support the position of the tandem but they may also be loaded with radioactive sources themselves.
• Vaginal, endometrial, and cervical cancers may be treated by either high- or lowdose-rate intracavitary implants. Replacing low-dose-rate (usually cesium) with high-dose-rate intracavitary brachytherapy treatments (usually iridium-192) is becoming increasingly common in the United States and Europe. High- dose-rate applications do not require anesthesia nor operating room time and radiation exposure is 10 to 20 minutes for each outpatient visit (usually four to six visits are required), whereas use of low-dose-rate cesium implants require hospitalization for 48 to 72 hours.
• Interstitial implants are another form of brachytherapy configured as radioactive wires or seeds and placed directly within tissues. Hollow guide needles are inserted in a geometric pattern to deliver a relatively uniform dose of radiation to a target tumor volume. After the position of the guide needles is confirmed, they can be threaded with the radioactive sources and the hollow guides removed. Interstitial implants are sometimes used in the treatment of locally advanced cervical cancer or for women with pelvic recurrences of endometrial or cervical cancer.
Common Side Effects of Radiation Therapy
• Dermatologic toxicity such as an acute skin reaction typically becomes evident by the third week of therapy. The reaction is characterized by erythema, desquamation, and pruritus and should resolve completely within 3 weeks of the end of treatment. Topical corticosteroids or moisturizing creams may be applied several times a day for symptomatic relief and to promote healing. If the reaction worsens, treatment is stopped and zinc oxide or silver sulfadiazine is applied to the affected area. The perineum is at greater risk for skin breakdown because of its increased warmth, moisture, and lack of ventilation. Therefore, patients should be instructed to keep the perineal area clean and dry. Additionally, late subcutaneous fibrosis can develop, especially with doses higher than 6,500 cGy.
• Hematologic toxicity is dependent on the volume of marrow irradiated and the total radiation dose. In adults, 40% of active marrow is in the pelvis, 25% is in the vertebral column, and 20% is in the ribs and skull. Extensive radiation to these sites may result in the need for blood product transfusions or administration of erythropoietin to support the patient's hematologic function during therapy.
• Gastrointestinal toxicity may be either acute or chronic. Nausea, vomiting, and diarrhea commonly occur 2 to 6 hours after abdominal or pelvic irradiation. Supportive therapy with hydration and administration of antiemetics and antidiarrheals are used for first-line therapy. In patients with severe diarrhea, opiates such as opium tincture, paregoric elixir, or codeine may be used to decrease peristalsis, whereas octreotide acetate (Sandostatin) may be given to reduce the volume of persistent high-output diarrhea. Occasionally, a reduction in fraction size or a break in treatment is necessary to control acute gastrointestinal side effects. Chronic diarrhea, obstruction caused by bowel adhesions, and fistula formation are serious complications of irradiation that occur in less than 1% of cases. Small bowel and rectovaginal fistulas can be caused by radiation effects or by recurrent disease. Once recurrence is ruled out as an etiology, the patient may require a temporary or permanent colostomy to allow healing of the affected bowel.
P.661
• Genitourinary toxicity typically presents as cystitis where the patient has pain, urgency, hematuria, and urinary frequency. The bladder is relatively tolerant of radiation, but doses higher than 6,000 to 7,000 cGy over a 6- to 7-week period can result in cystitis. The diagnosis of radiation cystitis may be made after a normal urine culture result has been obtained. Hydration, frequent sitz baths, and, possibly, the use of antibiotics and antispasmodic agents may be necessary for treatment. Hemorrhagic cystitis may lead to symptomatic anemia that requires blood transfusions and hospitalization. Clot evacuation of the bladder with continuous bladder irrigation is often necessary. Bladder irrigation with 1% alum or 1% silver nitrate can alleviate bleeding. Persistent bleeding on continuous bladder irrigation or significant gross hematuria in the unstable patient requires immediate cystoscopy to localize and control the bleeding.
• Vesicovaginal fistulas and ureteral strictures are possible long-term complications of radiation therapy. Placement of nephrostomies, insertion of ureteral stents, and, less commonly, surgical intervention may be necessary.
• Vulvovaginitis occurs secondary to erythema, inflammation, mucosal atrophy, inelasticity, and ulceration of the vaginal tissue. Adhesions and stenosis of the vagina are common and can result in pain on pelvic examination and intercourse. Treatment involves vaginal dilation, either by frequent sexual intercourse or with a vaginal dilator. In addition, the use of estrogen creams is useful in promoting epithelial regeneration. Infections, including candidiasis, trichomoniasis, and bacterial vaginosis, may be associated with radiation- induced vaginitis.
• The most common neurologic side effect is fatigue. This may continue for several months after completion of therapy. As with chemotherapy-induced fatigue, correction of anemia, good sleep hygiene, and regular exercise can help decrease fatigue.
OTHER ANTICANCER AGENTS
• Hormonal agents have been studied extensively in gynecologic cancer, including tamoxifen (which has both antiestrogenic effects in breast tissue as well as estrogen stimulatory effect in endometrial and myometrial tissues), medroxyprogesterone acetate (Provera), and progesterone-releasing intrauterine devices. These agents take advantage of the fact that both normal and well-differentiated neoplastic gynecologic tissues generally have both estrogen and progesterone receptors.
• These receptors are commonly lost as tumors become less well differentiated.
PRIMARY TREATMENT MODALITIES ACCORDING TO CANCER SITE
Epithelial Ovarian Cancer
• Women with epithelial ovarian cancer (EOC) need surgical staging to confirm the diagnosis and guide treatment planning. Patients with stage III and IV EOC require optimal surgical cytoreduction (residual tumor implants less than 1cm in diameter), either at time of initial surgery or after three to four cycles of neoadjuvant chemotherapy. Carcinoma of the fallopian tube and primary peritoneal carcinoma should be managed the same way as epithelial ovarian carcinoma.
• Patients with stage IA and IB, grades 1 to 2, disease do not benefit from adjuvant chemotherapy. Patients with stage IC, all grades, and those with stage IA and IB, grade 3, disease should receive three to six cycles of IV platinum-based adjuvant chemotherapy, which has been shown to improve both recurrence-free and overall survival.
P.662
• Patients with stages III and IV EOC should be treated with at least six cycles of platinum-taxane-based chemotherapy. As mentioned earlier, neoadjuvant chemotherapy may also be considered for patients unfit for surgery at the time of presentation due to extent of disease, comorbidities, or poor performance status. Women with stage III EOC who have minimal or no residual disease after primary surgery should receive combined IV and intraperitoneal (IP) chemotherapy. Although the combined IV/IP regimens are associated with greater neurologic, metabolic, and hematologic toxicity than IV regimens, there is significant improvement in both progression-free survival and overall survival associated with the combined IV/IP approach.
• EOCs that persist or progress despite surgery and primary platinum-based chemotherapy are termed “platinum refractory.” EOCs that recur within 6 months of the last platinum-based treatment are termed “platinum resistant,” whereas neoplasms that recur more than 6 months later than the last platinum-based treatment are considered “platinum sensitive.” Drugs commonly used for the treatment of women with platinum-refractory or platinum-resistant disease include topotecan, liposomal doxorubicin, docetaxel, gemcitabine, weekly paclitaxel, and bevacizumab. Patients with platinum-sensitive disease are generally treated with a combination of platinum and another active agent.
Ovarian Germ Cell Cancers
• As with EOC, comprehensive surgical staging is critical for patients with ovarian germ cell cancers. Young patients with stage I pure dysgerminoma and low-grade (grade 1) immature teratoma who wish to preserve fertility are adequately treated with unilateral salpingo-oophorectomy alone. All other patients with stage I to IV disease should undergo adjuvant chemotherapy with three courses of bleomycin, etoposide, and cisplatin after primary surgery. Postoperative radiation is an option for patients with dysgerminoma.
Cervical Cancer
• Surgery, chemotherapy, and radiation therapy all play a role in the management of women with cervical cancer limited to the pelvis (stages IA to IVA). Treatment options for a woman with stage IA1 cervical cancer include cervical conization and simple hysterectomy. For IA2 to IIA disease, options with similar benefit include radiation therapy and radical hysterectomy with bilateral pelvic lymphadenectomy. T reatment options for women with stage IIB to IVA disease include radiation, platinum-based chemoradiation, and neoadjuvant chemotherapy followed by radical hysterectomy.
• Radiation sensitization with concomitant cisplatin improves both progression-free and overall survival for women with cervical cancer. For women who cannot tolerate platinum, other chemosensitizing agents such as 5-fluorouracil (5-FU) can be considered. It is important to note, however, that patients who undergo both surgery and radiation (or chemoradiation) for the treatment of their cervical cancer will experience more short- and long-term toxicity than those who are treated with one modality alone.
• T reatment for women with stage IVB disease should focus on symptom control, as these patients are not curable with currently available treatment options. Radiation may be used for palliation of central disease and/or distant metastases. Drugs with known activity include cisplatin, ifosfamide, paclitaxel, irinotecan, and the twodrug combinations of cisplatin with ifosfamide, paclitaxel, or gemcitabine. Women
P.663 who experience a pelvic recurrence after primary surgery for cervical cancer should be considered for chemoradiation or pelvic exenteration, both of which have cure rates <50%. The same chemotherapeutic agents listed for women with stage IVB disease also may be considered for women with distant recurrent disease.
Vulvar Cancer
• The goals for treatment of vulvar cancer include efforts to decrease the extent of surgery and preserve normal urinary, rectal, and sexual functions while providing curative therapy. Early vulvar cancer (less than 1 mm deep) is treated with wide local excision. When the lesion is deeper than 1 mm and less than 2 cm from the midline, the patient is offered a radical local excision with bilateral inguinal node dissection. If greater than two lymph nodes return positive, the pelvic nodes are examined and radiation started. Locally advanced disease may be treated with neoadjuvant chemoradiation, radical vulvectomy and lymph node dissection, or exenteration. There is no effective chemotherapy identified for patients with distant metastatic vulvar cancer.
Vaginal Cancer
• Early vaginal cancer may be treated with either surgery or radiation (intracavitary with or without interstitial radiation). More advanced disease (stage II to IV) is generally treated with radiation alone. Platinum-based chemoradiation is also commonly used.
Endometrioid Endometrial Carcinoma
• Endometrioid endometrial carcinomas are thought to arise in the hormonal milieu of estrogen excess relative to progesterone. Prolonged progesterone therapy has been shown to induce histologic regression of cancer in about 50% to 78% of women with well-differentiated endometrioid endometrial carcinoma confined to the endometrium. Hormonal therapy, therefore, may be a treatment option among young women who wish to preserve fertility, as well as among patients with multiple comorbidities for whom the operative risks outweigh the benefits.
• Hysterectomy and bilateral salpingo-oophorectomy are the standard of care for women with stage I disease and radical hysterectomy and bilateral salpingo-oophorectomy for women with stage II disease. Pelvic and para-aortic lymphadenectomy are also advocated to complete surgical staging. Pelvic radiation, whether vaginal cuff brachytherapy or external beam radiation, should also be offered. Patients found to have metastatic disease at time of hysterectomy (stages III and IV) will benefit from platinum and taxane chemotherapy. Radiation directed at sites is offered to patients with adequate performance status.
• Patients found to have endometrial cancer recurring in the pelvis may benefit from surgical resection and radiation. Patients with distant metastatic disease should receive the same combination chemotherapy as those with stage III and IV disease. The small subset of women with recurrent grade I disease may benefit from hormonal therapy.
Uterine Carcinosarcomas
• The primary treatment for uterine carcinosarcomas is total abdominal hysterectomy, bilateral salpingo- oophorectomy, and lymphadenectomy. Adjuvant chemotherapy with ifosfamide and paclitaxel is recommended given improved progression-free and overall survival. Adjuvant pelvic radiation is often offered due to decreased risk of local recurrence, although overall survival is not impacted.
P.664
Uterine Leiomyosarcomas
• The primary treatment for leiomyosarcomas remains total abdominal hysterectomy and bilateral salpingo- oophorectomy. Adjuvant doxorubicin appears to offer a highresponse rate for primary treatment, whereas adjuvant pelvic radiation reduces the risk of local recurrence but does not improve overall survival. The most active agents for women with recurrent or metastatic disease include gemcitabine and docetaxel.
Gestational Trophoblastic Tumors
• Hydatidiform mole is treated with dilatation and curettage, although hysterectomy is advised if childbearing is completed. When persistent disease is suspected (serum human chorionic gonadotropin levels that rise or plateau), women are treated with either methotrexate with leucovorin or single-agent dactinomycin. Those with recurrent gestational trophoblastic tumors (GTT) after primary chemotherapy are treated with a five-drug combination of etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine (Oncovin). This combination is commonly abbreviated as EMA-CO. Hysterectomy may be indicated for patients with disease that persists after multidrug therapy. Women with recurrent GTT metastatic to the brain should be treated with both whole brain radiation therapy and chemotherapy with ifosfamide, carboplatin, and etoposide. Placental site trophoblastic tumors are not sensitive to chemotherapy; they should be treated with primary hysterectomy.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. Clinical management guidelines for obstetricians- gynecologists. ACOG practice bulletin no. 65: management of endometrial cancer. Obstet Gynecol
2005;106(2):413-425.
Baekelandt MM, Castiglione M; ESMO Guidelines Working Group. Endometrial carcinoma: ESMO recommendations for diagnosis, treatment and follow-up. Ann Oncol 2008;19(suppl 2): ii19-ii20.
Byrd LM, Swindell R, Webber-Rookes D, et al. Endometrial adenocarcinoma: an analysis of treatment and outcome. Oncol Rep 2008;20:1221-1228.
Chemotherapy for Cervical Cancer Meta-Analysis Collaboration. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: a systematic review and meta-analysis of individual patient data from 18 randomized trials. J Clin Oncol 2008;26:5802-5812.
Fiorelli JL, Herzog TJ, Wright JD. Current treatment strategies for endometrial cancer. Expert Rev Anticancer Ther 2008;8:1149-1157.
Gershenson DM. Management of ovarian germ cell tumors. J Clin Oncol 2007;25:2938-2943.
Greer BE, Koh WJ, Abu-Rustum N, et al. Cervical cancer. J Natl Compr Canc Netw2008;6(1): 14-36.
Haie-Meder C, Morice P, Castiglione M; ESMO Guidelines Working Group. Cervical carcinoma: ESMO recommendations for diagnosis, treatment and follow-up. Ann Oncol 2008; 19(suppl 2):ii17-ii18.
Kyrgiou M, Salanti G, Pavlidis N, et al. Survival benefits with diverse chemotherapy regimens for ovarian cancer: meta-analysis of multiple treatments. J Natl Cancer Inst 2006;98: 1655-1663.
Morgan RJ Jr, Alvarez RD, Armstrong DK, et al. Ovarian cancer: clinical practice guidelines in oncology. J Natl Compr Canc Netw2008;6:766-794.
Pectasides D, Kamposioras K, Papaxoinis G, et al. Chemotherapy for recurrent cervical cancer. Cancer Treat Rev 2008;34(7):603-613.
Reed NS. The management of uterine sarcomas. Clin Oncol (R Coll Radiol) 2008;20:470-478.
Temkin SM, Fleming G. Current treatment of metastatic endometrial cancer. Cancer Control 2009;16:38-45.