49 Gestational T rophoblastic Disease
Lauren Cobb
Robert L. Giuntoli II
Gestational trophoblastic disease (GTD) is a heterogeneous group of interrelated but distinct neoplasms derived from the trophoblastic cells of the placenta.
Lesions range from the premalignant complete and partial hydatidiform moles to the malignant invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT). Most women with GTD can be cured with their fertility preserved.EPIDEMIOLOGY OF GESTATIONAL TROPHOBLASTIC DISEASE AND TYPES OF TROPHOBLASTIC CELLS
• Incidence of GTD varies widely throughout the world, with the highest rates reported in Asia, Africa, and Latin America.
• In the United States, hydatidiform moles are observed in 1 in 600 therapeutic abortions and 1 in 1,000 to 1,200 pregnancies. Approximately 20% of patients require treatment for malignant sequelae after evacuation of hydatidiform mole.
• Gestational choriocarcinoma, by comparison, occurs in about 1 in 20,000 to 40,000 pregnancies.
• Although much less common than hydatidiform mole or choriocarcinoma, PSTT and ETT can develop after any type of pregnancy.
Risk Factors for Gestational T rophoblastic Disease
• Risks for GTD include:
• Extremes of reproductive age: Women older than age 40 years have a 5.2-fold increased risk, whereas women younger than age 20 years have a 1.5-fold increased risk. Persistent GTD occurs more frequently in older patients.
• History of previous hydatidiform mole: The risk of a subsequent hydatidiform mole rises by 10- to 20fold. With two previous molar pregnancies, the risk multiplies by 40-fold. Conversely, term pregnancies and live births produce a protective effect.
• Obstetric history of spontaneous abortions doubles the risk of molar gestation.
• Race: Asians and Latin Americans demonstrate a higher risk of being diagnosed with GTD, whereas North Americans and Europeans have lower risk.
• Low socioeconomic status and dietary factors such as vitamin A deficiency and low carotene intake may be associated, as well as cigarette smoking and oral contraceptive use. However, these associations are weak and not demonstrated consistently across all studies.
Types of Cells and Hormone Secretion
• T rophoblasts are specialized cells of the early blastocyst that play a role in implantation of the embryo and will eventually form the placenta.
• Three types of placental trophoblastic cells have been identified: cytotrophoblast, Syncytiotrophoblast, and intermediate trophoblast.
• Cytotrophoblasts comprise the inner layer of the trophoblast. They are primitive trophoblastic cells that are polygonal to oval in shape. They exhibit a single nucleus and clearly defined borders. Mitotic activity is evident, as these cells behave like stem cells. Implantation of the embryo is dependent on functioning cytotrophoblasts.
• Cytotrophoblasts do not produce either human chorionic gonadotropin (hCG) or human placental lactogen (hPL).
• Syncytiotrophoblasts comprise the outer layer of the trophoblast. They are Welldifferentiated cells that interface with the maternal circulation and produce most of the placental hormones. No mitotic activity is evident.
• Syncytiotrophoblasts demonstrate hCG production at 12 days of gestation. Secretion rapidly increases and peaks by 8 to 10 weeks, with a decline thereafter. By 40 weeks, hCG is present only focally in syncytiotrophoblasts. At 12 days, hPL is also present in syncytiotrophoblasts. Production continues to rise throughout pregnancy.
• Intermediate trophoblasts show infiltrative growth into decidua, myometrium, and blood vessels and in a normal pregnancy, they anchor the placenta to maternal tissue. Intermediate trophoblasts characteristically invade the wall of large vascular channels until the wall is completely replaced. Intermediate trophoblasts are the predominant cells of PSTT and exaggerated placental sites.
• As early as 12 days after conception, hCG and hPL are present focally in intermediate trophoblasts. However, at 6 weeks, hCG production disappears, whereas secretion of hPL peaks at 11 to 15 weeks' gestation.
CLASSIFICATION OF GESTATIONAL TROPHOBLASTIC DISEASE
Gestational trophoblastic neoplasms are unique among human neoplastic disorders because they are genetically related to fetal tissues. The molecular pathogenesis of these tumors is an area of active research interest.
Hydatidiform Mole
• In both partial and complete hydatidiform moles, the placental villi become edematous, forming small grape-like structures. Despite the cytogenetic, pathologic, and clinical differences in these disease processes (Table 491), the management of patients is similar.
• Ultrasound establishes the diagnosis, identifying a mixed echogenic pattern as villi and blood clots replace normal placental tissue. Medical complications occur in approximately 25% of patients, being more prominent in those with uterine enlargement >14 to 16 weeks' gestational size.
Complete Mole
• Clinical findings
• Presentation is between 11 and 25 weeks' gestation, with an average gestational age of 16 weeks.
• Vaginal bleeding is the most common presenting symptom, occurring in 97% of cases.
• Uterine size is often greater than expected for gestational age; however, in approximately one third of patients, the uterus is small for gestational dates. Ovarian enlargement caused by theca lutein cysts occurs in 25% to 35% of cases.
P.645
| TABLE 49-1 Comparison of Complete versus Partial Hydatidiform Mole | ||
| Complete | Partial | |
| Karyotype | Most commonly 46,XX or | Most commonly 69,XXX or |
| 46,XY | 69,XXY | |
| Uterine size | ||
| Large for gestational age | 33% | 10% |
| Small for gestational age | 33% | 65% |
| Diagnosis by ultrasonography | Common | Rare |
| Theca lutein cysts | 25%-35% | Rare |
| β-hCG (mIU/mL) | >50,000 | mIU/mL.
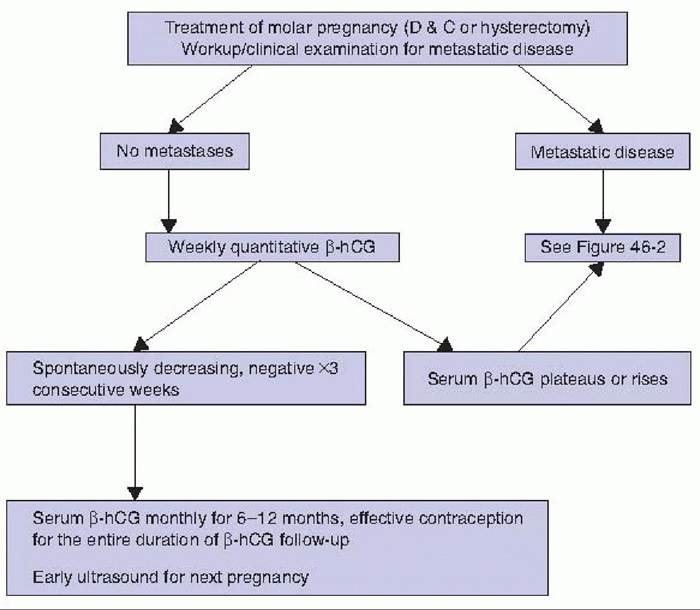
• Severe hyperemesis and pregnancy-induced hypertension can develop in up to 25% of women, with hyperthyroidism in 7% of cases (hCG has weak thyroidstimulating activity secondary to some homology between the beta subunits of thyroid-stimulating hormone and hCG). • Ultrasonography often, but not always, shows a classic “snowstorm” appearance. • Pathologic features • Gross findings include massively enlarged, edematous villi that give the classic grape-like appearance to the placenta and lack embryonic tissue. • Microscopic examination shows hydropic swelling in the majority of villi, accompanied by a variable degree of trophoblastic proliferation. Complete moles have widespread, diffuse immunostaining for hCG; moderately diffuse staining for hPL; and focal staining for placental alkaline phosphatase (PLAP). • Chromosomal abnormalities Most complete moles are diploid, with a 46,XX karyotype; rare examples of triploid or tetraploid moles have been reported. • In most cases, all of the chromosomal complements are paternally derived. The XX genotype typically results from duplication of a haploid sperm pronucleus in an empty ovum. Three percent to 13% of complete moles have a 46,XY chromosome complement, presumably as a result of dispermy, in which an empty ovum is fertilized by two sperm pronuclei. Incomplete Mole • Clinical findings • Commonly, patients present between 9 and 34 weeks' gestation. • These tumors are consistently associated with embryonic/fetal tissue. • Patients report abnormal uterine bleeding in about 75% of cases. A clinical diagnosis of a missed or spontaneous abortion is made in 91% of women with incomplete molar pregnancy. • Uterine size is generally small for gestational dates; excessive uterine size is observed in less than 10% of patients. P.646 • Serum hCG level is in the normal or low range for gestational age. • Preeclampsia occurs with lower incidence (2.5%) and presents much later with a partial mole than with a complete mole but can be equally severe. • Pathologic features • Gross findings reveal fetal tissue in nearly all instances, although its discovery may require careful examination because early fetal death normally takes place (i.e., 8 to 9 weeks' gestational age). • Microscopic examination finds two populations of chorionic villi: one of normal size and the other grossly hydropic. Partial moles show focal to moderate immunostaining for hCG and diffuse staining for hPL and PLAP. • Chromosomal abnormalities • Karyotype of partial moles most frequently shows triploidy (i.e., 69 chromosomes), with two paternal and one maternal chromosome complement. • The chromosomal complement is XXY in 70% of cases, XXX in 27% of cases, and XYY in 3% of cases. The abnormal conceptus in these cases arises from the fertilization of an egg with a haploid set of chromosomes either by two sperm, each with a set of haploid chromosomes, or by a single sperm with a diploid 46,XY complement. Invasive Mole • Invasive mole is an important complication of hydatidiform mole, representing 70% to 90% of cases of persistent GTD. Other common names include chorioadenoma destruens, penetrating mole, malignant mole, or molar destruens. • Pathologic features • Histologically, hydropic chorionic villi migrate into the myometrium, vascular spaces, or outside of the pelvis in 20% of cases to the vagina, perineum, or lungs. • Grossly, invasive moles present as erosive, hemorrhagic lesions extending from the uterine cavity into the myometrium. Metastasis can range from superficial penetration to extension through the uterine wall, with subsequent perforation and life-threatening hemorrhage. Molar vesicles are often apparent. • Microscopically, the diagnostic feature of invasive mole is the presence of molar villi and trophoblast within the myometrium or at an extrauterine site. Lesions at distant sites are usually composed of molar villi confined within blood vessels, without invasion into adjacent tissue. Choriocarcinoma • Gestational choriocarcinoma is a highly malignant epithelial tumor that can be associated with any type of gestational event, most often a complete hydatidiform mole. In the United States, choriocarcinoma occurs in 1 in 20,000 to 40,000 pregnancies. Approximately 25% of gestational choriocarcinomas develop after term pregnancies, 50% after molar gestations, and 25% after abortion or ectopic pregnancies. Early systemic hematogenous metastasis often takes place.• Clinical findings • Eighty percent of patients with extrauterine disease show pulmonary metastases, whereas approximately 30% demonstrate extension to the vagina. Ten percent of women also exhibit liver and central nervous system involvement. • Pathologic features • On gross examination, these tumors appear as dark red, hemorrhagic masses with shaggy, irregular surfaces. Metastatic lesions outside the uterus are well circumscribed. P.647 On microscopic examination, sheets of syncytiotrophoblasts and cytotrophoblasts are seen without chorionic villi, invading surrounding tissue or permeating vascular spaces. Placental Site and Epithelioid T rophoblastic T umor • PSTT and ETT are rare gestational trophoblastic neoplasms, accounting for 1% of persistent GTD. Both can develop long after prior gestational events. Most cases of PSTT and ETT are benign, especially those tumors that are confined to the uterus, but about 15% to 25% of cases are malignant and present with local invasion and distant metastasis. • Clinical features • PSTTs and ETTs usually remain confined to the uterus and metastasize late. In some cases, recurrent or metastatic PSTT/ETTs can occur in patients long after initial treatment. • These tumors typically produce only small amounts of β-hCG, despite a large tumor burden. Serum hPL, produced by the intermediate trophoblasts that predominate, serves as a better marker for disease progression or recurrence. • Approximately 15% of lesions metastasize to extrauterine sites (e.g., lungs, liver, abdominal cavity, and brain). In contrast to other trophoblastic tumors, these tumors are relatively insensitive to chemotherapy, and surgical excision is usually the best treatment modality. • Pathologic features • By contrast to the normal implantation site, where invasion of the extravillous subtype of intermediate trophoblast is tightly regulated and confined to the inner third of the myometrium, tumor cells of PSTT and ETT are invasive and infiltrate deeply into the myometrium. • Although PSTT and ETT share similar clinical features, careful examination of tumor histology and gene expression patterns shows that PSTT and ETT are composed of different extravillous trophoblastic cells. • Gross lesions may be barely visible or may result in diffuse nodular enlargement of the myometrium. Most tumors are well circumscribed. Microscopically, invasion may extend to the uterine serosa and, in rare instances, extends to adnexal structures. DIAGNOSIS AND MANAGEMENT OF MOLAR PREGNANCY • The pathologic diagnosis of hydatidiform mole is typically made following dilation and curettage (D&C) performed for an incomplete abortion or because of suspicion of hydatidiform mole based on clinical findings. • The following tests should be performed preoperatively: î Quantitative serum β-hCG level î Complete blood count î Prothrombin time, partial thromboplastin time î Comprehensive metabolic panel with renal and liver function tests î Blood type and screen î Rh-negative patients must be given RhO (D) immunoglobulin (RhoGAM) î Chest radiograph • The primary treatment for hydatidiform mole is suction D&C. • The following steps should be taken before suction D&C: î Stabilization of medical complications î Full operating room support in a hospital setting î Large-bore intravenous (IV) access with possible central line monitoring P.648 î Induction of regional or general anesthesia î Initiation of oxytocin drip (during D&C) • Uterine evacuation is accomplished with the largest cannula that can be safely introduced through the cervix. IV oxytocin is begun after the cervix is dilated and suction is initiated and is continued postoperatively for several hours. • Postevacuation follow-up should include: • β-hCG level 48 hours after evacuation • Weekly β-hCG level until three consecutive negative results, then monthly until results are negative for 6 consecutive months (Fig. 49-1) • Regular pelvic examinations to monitor involution of pelvic organs and for detection of metastasis • Repeat chest radiograph if the β-hCG titer plateaus or rises. • Effective contraception for the entire interval of β-hCG follow-up testing. Preventing pregnancy is crucial, as a rising β-hCG titer due to a normal pregnancy cannot be distinguished from persistent GTD. • Because of increased risk (1 % to 2%) of a second mole in subsequent pregnancies, all future pregnancies should be evaluated by ultrasonography early in their course. • Complications include anemia, infection, hyperthyroidism, pregnancy-induced hypertension or preeclampsia, and theca lutein cysts.
Figure 49-1. Follow-up of molar pregnancy. D&C, dilation and curettage; β-hCG, beta-human chorionic gonadotropin. (Adapted from American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. ACOG practice bulletin no. 53: diagnosis and treatment of gestational trophoblastic disease. Obstet Gynecol 2004;103:1365-1377.) P.649 DIAGNOSIS AND MANAGEMENT OF PERSISTENT GESTATIONAL TROPHOBLASTIC DISEASE Persistent GTD includes invasive mole, choriocarcinoma, and PSTT. Persistent disease occurs in approximately 20% of cases of complete mole; approximately 15% develop invasive GTD and 10% for three measurements over a 2-week duration (days 1, 7, and 14) • Detectable hCG for >6 months after molar evacuation • Histologic diagnosis of choriocarcinoma • The diagnosis of persistent GTD is based on the quantitative pattern of serum β-hCG level, D&C findings, presence of metastatic disease, and histology. Both invasive mole and choriocarcinoma are typically detected by a plateau or elevation in the β-hCG titer. It may not be possible to distinguish clinically between these lesions. • Obtaining a tissue diagnosis is not necessary (because the treatment for both is the same) and may be associated with significant hemorrhage. PSTTs and ETTs typically demonstrate low β-hCG levels; however, serum hPL level is often elevated and may be a more useful serologic marker. • All patients suspected of having persistent GTD should undergo the following workup to evaluate the extent of disease (Fig. 49-2): • Complete history and physical examination • Serum β-hCG level, possibly serum hPL level • Liver, thyroid, and renal function tests • Complete blood count • Pelvic ultrasonography to evaluate for intrauterine pregnancy • Chest radiograph • Computed tomography of pelvis, abdomen, and brain • Stool guaiac test P.650
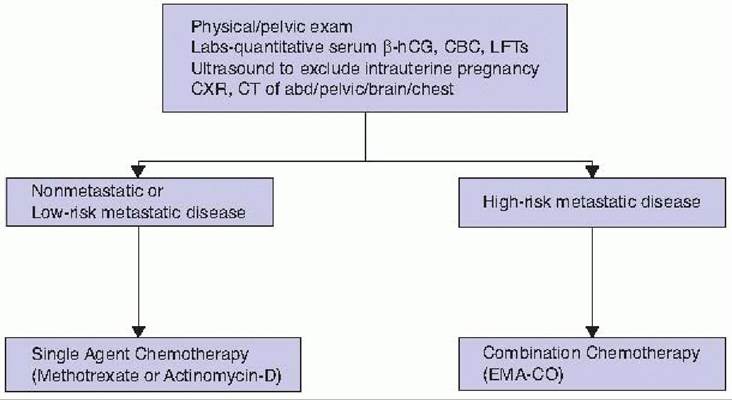
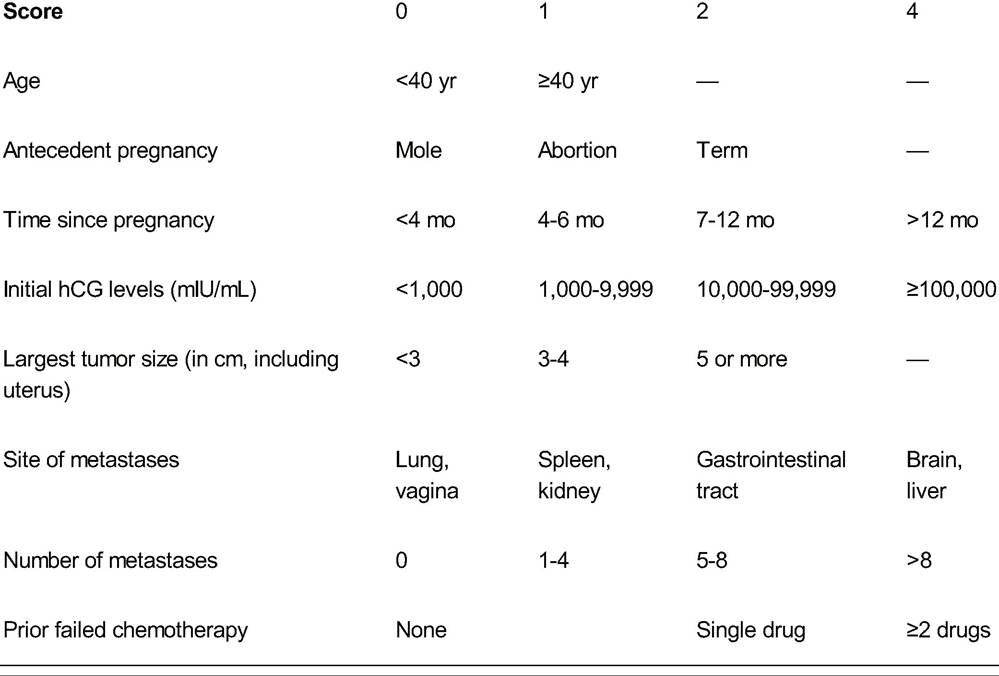
Figure 49-2. Management of persistent GTD. β-hCG, beta-human chorionic gonadotropin; CBC, complete blood count; LFT, liver function test; CXR, chest radiograph; CT, computed tomography; EMA-CO, etoposide, methotrexate, actinomycin D, cyclophosphamide (Cytoxan), and vincristine sulphate. (Adapted from American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. ACOG practice bulletin no. 53: diagnosis and treatment of gestational trophoblastic disease. Obstet Gynecol 2004;103:1365- 1377.) Treatment of Persistent Gestational Trophoblastic Disease • Treatment depends on the stage of disease (Table 49-2) and risk assessment based on the World Health Organization (WHO) prognostic scoring system (Table 49-3). TABLE 49-2 International Federation of Gynecology and Obstetrics Staging System for Gestational Trophoblastic Neoplasia Stage Description I Strictly confined to uterus II Extension outside uterus but limited to pelvic structures III Extension to lungs IV All other metastatic sites Each stage is divided into high or low risk using the World Health Organization prognostic scoring index. From FIGO Committee on Gynecologic Oncology. Current FIGO staging for cancer of the vagina, fallopian tube, ovary, and gestational trophoblastic neoplasia. Int J Gynecol Obstet 2009;105:3-4. Nonmetastatic Disease and Low-Risk Metastatic Disease • Disease falls into the category of low risk based on a WHO prognostic score ≤6. • Primary treatment is with single-agent chemotherapy with either methotrexate (MTX) or actinomycin D. • MTX is alternated with folinic acid in most institutions and given with a fixed window of 7 to 14 days between courses. Some evidence suggests that dactinomycin may provide slightly higher remission rates than MTX but is P.651 associated with more toxicity. Pulsed dactinomycin (higher dose administered every 2 weeks) generally is used more frequently than the 5-day regimen. • Systemic treatments are administered until hCG levels normalize for two or more consecutive assessments. An additional one to three cycles of consolidation chemotherapy can be given after a negative serum hCG is obtained. • If hCG titers plateau or rise after two courses, the patient is considered resistant to that particular chemotherapeutic agent, and the alternative single-agent chemotherapy is promptly instituted. If no response is seen after both single agents, then combination chemotherapy is required. • For patients who have completed childbearing, hysterectomy should be considered for refractory disease confined to the uterus. • For patients with stage I or II PSTT, the primary treatment is hysterectomy, especially given the wide variation in response of PSTT to chemotherapy. • Patients with nonmetastatic disease are less likely to require second-line therapy than patients with low-risk metastatic disease. Overall, 85% to 95% of patients can be cured with single-agent chemotherapy without hysterectomy. The cure rate for patients with low-risk disease approaches 100% with recurrence rates 49-3 International Federation of Gynecology and ObstetricsZWorld Health Organization Prognostic Scoring Index for Gestational Trophoblastic Neoplasia
The total score is obtained by adding the scores for individual prognostic factors. Scores from 0 to 6 are categorized as low risk, whereas a score of 7 or higher is high risk. Adapted from Kohorn EI. The new FIGO 2000 staging and risk factor scoring system for gestational trophoblastic disease: description and clinical assessment. Int J Gynecol Cancer 2001 ;11:73-77. High-Risk Metastatic Disease • Disease may be deemed high risk based on a WHO prognostic score ≥7. • For patients with high-risk metastatic disease, the recommended treatment is combination chemotherapy with etoposide, MTX, actinomycin D, cyclophosphamide (Cytoxan), and vincristine sulfate (EMA-CO). Recurrent or refractory disease, P.652 particularly in cases of chemoresistant PSTT and ETT, may respond better to platinum-etoposide combinations such as etoposide, methotrexate, actinomycin, and cisplatinum (EMA-EP). • EMA-CO is administered every 2 weeks until remission (negative hCG levels are achieved in 3 consecutive weeks) or until intolerable side effects occur. After the normalization of hCG levels, an additional three courses should be given as consolidation therapy. • For patients with complications of metastatic disease specific to the organ involved, the following interventions can be instituted: • Vaginal involvement: These lesions can bleed profusely. Bleeding can be controlled with packing for 24 hours. Prompt radiation to the affected region may provide further hemostasis. Although infrequently used, embolization of the pelvic vessels may also be implemented in women with life-threatening or recurrent hemorrhage. • Pulmonary metastases: These lesions usually respond to chemotherapy. Occasionally, thoracotomy is required to remove a persistent viable tumor nodule. Not all chest lesions clear radiographically due to scarring and fibrosis from the injury and healing process. • Hepatic lesions: If these lesions fail to respond to systemic chemotherapy, other options include hepatic arterial infusion of chemotherapy or partial hepatic resection to remove resistant tumor. These lesions are usually hypervascular and prone to hemorrhage if biopsied. • Cerebral metastases: Whole brain irradiation (approximately 3,000 cGy) is initiated as soon as the extent of disease is confirmed. Radiation and chemotherapy reduce the risk of spontaneous cerebral hemorrhage. However, concurrent whole brain radiation and chemotherapy increase treatment-related toxicity, especially leukoencephalopathy (radiographic diffuse white matter changes with symptoms of lethargy, seizures, and dysarthria and rarely ataxia, dementia, memory loss, and death). Alternatively, cerebral metastases can be treated with high-dose EMA-CO with or without intrathecal MTX. • Extensive uterine disease: Hysterectomy is indicated in cases with large intrauterine tumor burden, infection, or hemorrhage. • Following EMA-CO, the overall remission rate is 80% to 90%. Approximately 25% of high-risk patients demonstrate incomplete responses to first-line therapy and relapse. When brain metastases are present, the overall remission rate drops to 50% to 60%. Higher failure rates are also seen with stage IV disease, greater than eight metastatic lesions, and a history of previous chemotherapy. • For patients with refractory or recurrent disease after EMA-CO treatment, salvage therapies often consist of platinum-etoposide combinations. Bleomycin and ifosfamide (etoposide, ifosfamide, and cisplatin [VIP]; ifosfamide, carboplatin, and etoposide [ICE]) have also been used with limited success. Experimental protocols may be investigated in these patients. SUGGESTED READINGS Berkowitz RS, Goldstein DP. Gestational trophoblastic disease. In Berek JS, ed. Berek and Novak’s Gynecology, 15th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2012. Hoffman BL, Schorge JO, Schaffer JI, et al, eds. Gestational trophoblastic disease. In Williams Gynecology, 2nd ed. New York, NY: McGraw-Hill, 2012.
More medical literature on Medic.Studio
More on the topic 49 Gestational T rophoblastic Disease:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|