48 Ovarian Cancer
Jill H. Tseng
Edward J. Tanner III
Ovarian cancer is the 10th most common cancer and the fifth leading cause of cancer-related death in American women. Ovarian cancer is the second most common gynecologic cancer following cancer of the uterine corpus and has the highest mortality of all female reproductive system malignancies.
EPIDEMIOLOGY OF OVARIAN CANCER
• For women in the United States, the lifetime risk of developing ovarian cancer is estimated to be 1 in 72 (1.4%). This likelihood increases with age, with a median age at diagnosis of 63 years.
• The risk of malignancy in a solid adnexal mass is 7% in a premenopausal woman and increases to 30% in a postmenopausal woman. Each year, an estimated 22,240 women will be diagnosed with ovarian cancer and 14,030 will die from their disease.
• Ovarian neoplasms, of which 80% are benign, are divided into three major groups: epithelial, germ cell, and sex cord-stromal tumors (T able 48-1). The ovary can also be a site of metastatic cancer from other sites, particularly from the breast or the gastrointestinal tract (e.g., Krukenberg tumors).
EPITHELIAL OVARIAN TUMORS
• T umors derived from the coelomic epithelium are the most common ovarian neoplasms, accounting for 65% of ovarian neoplasms and 90% of ovarian cancers.
• Histologic types include serous, mucinous, endometrioid, clear cell, and transitional (Brenner).
Risk Factors
• Age older than 40 years, white race, nulliparity, infertility, history of endometrial or breast cancer, and family history of ovarian cancer have been consistently found to increase the risk of invasive epithelial cancer. Increased parity, use of oral contraceptive pills (OCPs), history of breast-feeding, tubal ligation, and hysterectomy have been associated with a decreased risk of ovarian cancer.
• Patients with a family history of ovarian, breast, endometrial, or colon cancer are at increased risk of developing ovarian carcinoma.
• Hereditary familial ovarian cancer accounts for approximately 10% of all newly diagnosed cases. Women with one first-degree relative with ovarian cancer have a 5% lifetime risk of developing the disease and those with two first- degree relatives with ovarian cancer have a 7% risk.
• There are three distinct autosomal dominant syndromes that have been termed familial ovarian cancer: sitespecific ovarian cancer, breast-ovarian cancer (BRCA1 and BRCA2), and hereditary nonpolyposis colorectal cancer (HNPCC or Lynch syndrome II).
P.626
TABLE 48-1 Classification of Ovarian Neoplasms
Epithelial Tumors
Serous (histology resembles the lining of the fallopian tube)
Mucinous (histology resembles endocervical epithelium)
Endometrioid (histology resembles endometrial lining)
Clear cell (histology resembles vaginal mucosa)
Transitional cell (Brenner; histology resembles bladder)
Germ Cell Tumors
Dysgerminoma
Endodermal sinus tumor
Embryonal carcinoma
Polyembryoma
Choriocarcinoma
Teratoma:
■ Immature
■ Mature
Sex Cord-Stromal Tumors
Granulosa-stromal cell
■ Granulosa cell
■ Thecoma-fibromas
Sertoli-Leydig cell
Sex cord tumor
Sex cord tumor with annular tubules
Gynandroblastoma
Unclassified and Metastatic
• HNPCC, also known as Lynch syndrome II, is an autosomal dominant cancer susceptibility syndrome that describes a familial predisposition to multiple cancers (primarily colon and also endometrial, ovarian, and genitourinary tract).
• Women with HNPCC have a 40% to 60% lifetime risk for endometrial cancer and a 12% lifetime risk for ovarian cancer. Mutations in three DNA mismatch repair genes, MLH1, MSH2, and MSH6, account for over 95% of
mutations found with Lynch syndrome.
• BRCA: Two breast and ovarian cancer susceptibility genes (BRCA1, located on chromosome 17q, and BRCA2, located on chromosome 13q) have been identified. These genes, which are involved in DNA repair, have been linked to familial breast cancer, breast-ovary, and site-specific ovarian cancer syndromes.
• Women with BRCA gene mutations have a lifetime breast cancer risk of 82%. The lifetime ovarian cancer risks of BRCA1 and BRCA2 carriers are 25% to 60% and 15% to 25%, respectively. These women also develop the disease at an earlier age than women without mutations. Genetic screening tests are available.
• Environmental factors may play a role in ovarian cancer. A recent meta-analysis does not support a causal relationship between talc exposure and ovarian cancer.
P.627
• Reproductive factors play an important role in ovarian cancer risk. Increasing parity is associated with a decreased relative risk of developing ovarian cancer, whereas nulliparity is associated with an increased risk.
• The use of OCPs also has been associated with a decreased relative risk.
• Women with a history of breast-feeding have a lower risk of ovarian cancer than nulliparous women and parous women who have not breast-fed.
• Women with infertility have an elevated risk of ovarian cancer, independent of nulliparity.
• Although fertility drugs have been implicated in the development of ovarian cancer, their association has not been clearly separated from the risk that nulliparity and infertility confer.
• Tubal ligation and hysterectomy with ovarian preservation both appear to lower the risk of ovarian cancer, although the mechanisms remain unclear.
Screening and Prevention
• Early ovarian cancer is often asymptomatic. No available screening test has sufficient positive predictive value for early-stage ovarian cancer.
• Routine yearly pelvic examination is currently recommended for the general population as a screening tool, but it has poor sensitivity for detecting early disease.
• Cancer antigen 125 (CA-125) is a biomarker for ovarian cancer. A level >35 U/mL in postmenopausal women is usually considered abnormal. Approximately 50% of ovarian cancer cases confined to the ovary, and >85% of advanced ovarian cancer cases have elevated CA-125 levels. However, this biomarker alone is neither sufficiently sensitive nor specific enough to be diagnostic for ovarian cancer.
• CA-125 levels may be elevated in several benign conditions (including pelvic inflammatory disease, endometriosis, fibroids, pregnancy, hemorrhagic ovarian cysts, liver disease, and any other lesion that causes peritoneal irritation) as well as in other malignant conditions (including breast, lung, pancreatic, gastric, and colon cancer). In addition, CA-125 is normal in approximately half of women with stage I ovarian cancer. The most important use is following serial CA-125 levels to monitor response to treatment and to detecting recurrence in women with known ovarian cancer.
• Human epididymis protein 4 (HE4) has similar sensitivity to CA-125 when ovarian cancer patients are compared to healthy controls; however, it has greater sensitivity when compared to those with benign gynecologic disease. Although not yet used for screening, HE4 is currently approved in the United States for monitoring disease progression or recurrence.
• Other biomarkers: CA 19-9, CA 15-3, CA 72-4, carcinoembryonic antigen, lysophosphatidic acid, sFas, mesothelin, haptoglobin-alpha, bikunin, HE4, and OVX1 are and have been investigated with combined biomarker tests commercially available for use in high-risk patients.
• Transvaginal ultrasonography has been evaluated as a potential screening tool. Characteristics suggestive of malignancy include complex ovarian cysts with solid components, the presence of septations, papillary projections into the cyst, thick cyst walls, surface excrescences, ascites, and neovascularization. When used to screen the general population, transvaginal ultrasonography has a poor positive predictive value. However, when limited to postmenopausal women with pelvic masses, a sensitivity of 84% and specificity of 78% has been reported.
• Multimodal screening using CA-125 measurement with transvaginal ultrasonography yields a higher specificity and positive predictive value than either modality alone. In postmenopausal women, the combination of transvaginal ultrasound
P.628 and a CA-125 >65 U/mL increased sensitivity to 92% and specificity to 96%.
However, the role of multimodal screening remains unclear.• A large prospective screening study, the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, found that concurrent multimodal screening did not reduce ovarian cancer mortality. Another ongoing large randomized trial, the United Kingdom Collaborative T rial of Ovarian Cancer Screening, demonstrated sequential multimodal screening (abnormal CA-125 followed by transvaginal ultrasound) to have a much greater sensitivity for primary ovarian and tubal cancers compared to transvaginal ultrasound alone in the initial years of screening. Final results are not expected until 2015. For this reason, additional studies are needed to determine the appropriateness of multimodal screening for ovarian cancer at this time.
• Current recommendations for screening: According to the U.S. Preventive Services Task Force, no existing evidence suggests that any screening test, including CA-125, ultrasound, or pelvic examination, reduces mortality from ovarian cancer; therefore, routine screening is not recommended. The American College of Obstetricians and Gynecologists (ACOG) agrees that routine screening tests are not beneficial for low-risk, asymptomatic women. ACOG advises the obstetriciangynecologist to remain vigilant for the early signs and symptoms of ovarian cancer. The American Cancer Society does not recommend routine screening but states that women at high risk of ovarian cancer should be offered the combination of a pelvic exam, transvaginal ultrasound, and CA-125.
• Prophylactic bilateral salpingo-oophorectomy: Women older than age 45 years who are undergoing any pelvic surgery may consider prophylactic removal of the ovaries and fallopian tubes. A bilateral salpingo-oophorectomy will essentially eliminate the risk for developing ovarian cancer, although a small risk of developing primary peritoneal cancer still remains. The sequelae of surgical menopause must be weighed against the potential benefit of averting ovarian malignancy.
• For this reason, there is no commonly agreed upon age at which bilateral salpingooophorectomy is recommended for normal-risk women, although studies have shown that prophylactic oophorectomy prior to age 45 years may decrease life span and risk of all-cause mortality.
• Women at high risk of ovarian cancer (e.g., Lynch syndrome, BRCA mutations) should consider prophylactic bilateral salpingo-oophorectomy when childbearing is complete.
• OCP prophylaxis is the only documented method of chemoprevention for ovarian cancer, and the effect is substantial. The overall estimate of protection with OCPs is approximately 40%. Increased duration of use appears to be associated with further decreased risk, and the protective effect persists for 10 or more years after discontinuation. The use of OCPs in BRCA mutation carriers also confers a decreased risk of ovarian cancer without increasing the risk of breast cancer.
Presentation and Diagnosis
• Presentation: Only 19% of ovarian cancer cases are diagnosed while the cancer is localized (stage I), and approximately 68% of patients with epithelial ovarian cancer have advanced disease (stage III or greater) at time of diagnosis. Although some women with early disease experience symptoms, the majority are
asymptomatic.
• When symptoms develop, they are nonspecific and can include abdominal bloating, early satiety, weight loss, constipation, anorexia, urinary frequency, dyspareunia, fatigue, and irregular menstrual bleeding.
P.629
TABLE 48-2 Risks of Specific Types of Cancers Associated with Autosomal Dominant Genetic Risk Syndromes
| Genetic Syndrome | BRCA1 | BRCA2 | HNPCC |
| T ype of Cancer | |||
| Ovarian cancer | 25%-60% | 15%-25% | 12% |
| Breast cancer | 82% | 82% | Not associated |
| Endometrial cancer | Not associated | Not associated | 40%-60% |
| Colon cancer | Possibly increased risk | Not associated | 70%-80% |
| Stomach cancer | Not associated | Possibly increased risk | 20% |
HNPCC, hereditary nonpolyposis colorectal cancer.
• On physical examination, a pelvic mass is an important sign of disease. In more advanced stages, abdominal distention may develop, and chest examination may reveal evidence of pleural effusion.
• Workup: Evaluation of a pelvic mass varies depending on the patient's age, significant medical and family history, and the sonographic characteristics of the mass. Women with pelvic masses that are suspicious for malignancy should be referred to a gynecologic oncologist (Table 48-2). In premenopausal women, an adnexal mass the pelvis, gutters, and diaphragm
Systematic exploration of all organs and surfaces
Hysterectomya
Bilateral salpingo-oophorectomya
Infracolic omentectomy
Sampling pelvic and para-aortic lymph nodes
Multiple biopsy specimens from peritoneal sites
Pelvic side walls
Surfaces of the rectum and bladder
Cul-de-sac
Lateral abdominal gutters
Diaphragm
aMay be preserved in select patients, particularly if future fertility is desired.
From Young RC, Decker DG, Wharton JT, et al. Staging laparotomy in early ovarian cancer. JAMA 1983;250(22):3072-3076; T rimbos JB, Schueler JA, van Lent M, et al. Reasons for incomplete surgical staging in early ovarian carcinoma. Gynecol Oncol 1990;37:374-377.
• Transitional cell tumors histologically resemble the bladder. The two types of malignant transitional cell tumors are Brenner tumors and transitional cell carcinomas. Approximately 10% to 20% of advanced-stage ovarian carcinomas contain a transitional cell carcinoma component. The mean age for malignant Brenner tumors is 63 years.
• Grade is an important independent prognostic factor, particularly in patients with early-stage disease.
• Based on a combination of architecture (glandular, papillary, or solid), degree of nuclear atypia, and mitotic index.
• Grade 1 is well differentiated, grade 2 is moderately differentiated, and grade 3 is poorly differentiated.
• More recently, a two-tiered grading system has been proposed. Low-grade tumors exhibit a low degree of atypia with infrequent mitotic figures and are thought to develop from adenofibromas or borderline tumors in a slow, stepwise process. High-grade tumors demonstrate atypical nuclei and numerous mitotic figures. These tumors are thought to develop rapidly de novo.
• Tumor ploidy has been demonstrated to be an independent prognostic variable. Diploid tumors are often stage IA, whereas aneuploid tumors are seen in more advanced cancer.
• Debulking, also called cytoreduction, is defined as removal of as much tumor as possible during surgical exploration. Optimal cytoreduction implies that any
P.633 remaining tumor nodules are less than 1 cm in diameter. Cytoreduction of all visible disease is associated with the greatest survival advantage, reinforcing the importance of a gynecologic oncologist involvement of primary diagnostic and cytoreductive surgery.
Management of Epithelial Ovarian Cancer
• Treatment of epithelial ovarian cancer depends on the stage and grade of the disease, type of disease (i.e., primary or recurrent), previous treatment, and the patient's performance status.
Tumors of Low Malignant Potential
• These tumors show a different pattern of behavior than do malignant ovarian disease. Approximately 15% of all epithelial ovarian tumors are classified as LMP and are often found in younger patients. They are most commonly of serous histology (85%) followed by mucinous.
• Serous LMP tumors with invasive implants tend to behave as low-grade carcinomas with a mortality rate of 34%.
• Mucinous LMP tumors confined to the ovary have a survival rate approaching 100%, whereas those with advanced- stage disease have a survival rate of 40% to 50%. They may be associated with a concurrent appendiceal primary tumor, and affected patients should also undergo appendectomy. Mucinous LMPs that display aggressive behavior are associated with pseudomyxoma peritonei, which is indicative of appendiceal origin.
• Surgical staging of LMPs is advocated because of the possibility of identifying an invasive cancer on final pathology. Because of their indolent growth, adjuvant therapy is not recommended even in patients with advanced disease.
• If disease recurs, it does so an average of 10 years after initial diagnosis, and resection can be performed again at the time of recurrence. Most patients die with the disease rather than from the disease.
• In addition, early-stage disease in women who desire future fertility may be treated with unilateral salpingo- oophorectomy, or even with unilateral cystectomy, with good outcomes.
Early Invasive Disease (Stage I or II)
• Initial surgical resection is necessary for establishing a histologic diagnosis and appropriate staging. Options exist for young patients who wish to preserve fertility. If intraoperative findings are consistent with stage I disease and the contralateral ovary is normal in appearance, unilateral salpingo-oophorectomy with thorough surgical staging may be performed. The uterus and normal-appearing contralateral ovary may remain in situ. The patient should be counseled about the potential for a second primary in the preserved ovary, and a total abdominal hysterectomy with removal of the remaining tube and ovary should be considered after childbearing is completed.
• Chemotherapy: For patients with stage IA, grade 1 or 2 disease, chemotherapy is not required. For patients with early-stage disease with prognostic factors placing them at higher risk for recurrence (stage IC or II, grade 3 disease, or clear cell histology of any stage), postoperative chemotherapy is recommended. Although platinumbased regimens are most commonly used, the optimal chemotherapy regimen for patients with early-stage disease is still being evaluated.
P.634
• Radiation: With relatively effective chemotherapeutic options available as well as frequency of widespread metastasis, radiation therapy is used infrequently in the treatment of ovarian cancer.
Advanced Invasive Disease
• Advanced disease requires surgical staging, debulking, and a course of platinumbased chemotherapy.
• Primary cytoreductive surgery, or debulking, is central in the treatment of advanced disease because optimal cytoreduction is one of the most powerful predictors of survival in patients with advanced ovarian cancer.
• The determination of residual disease upon completion of the procedure does not include the total volume of tumor cells left behind but rather the diameter of the largest single residual nodule. For example, a patient with one unresected nodule measuring 2.5 cm has not undergone optimal debulking, whereas debulking is considered to be optimal in a patient with residual miliary studding of the entire peritoneal cavity.
• Neoadjuvant therapy, treatment prior to surgery, has been associated with a lower overall survival compared to initial surgery. However, it may be an appropriate alternative for patients whose performance status prohibits initial surgery. In addition, for patients in whom suboptimal debulking is likely, neoadjuvant chemotherapy has been used as an alternate strategy prior to surgery in an attempt to increase the likelihood of optimal tumor debulking.
• Combination chemotherapy is most often used as postoperative (adjuvant) treatment for advanced epithelial ovarian cancer. Combination chemotherapy with six cycles of carboplatin plus paclitaxel is the treatment of choice for patients with advanced disease. One cycle is given every 3 weeks, with monitoring of tumor status by physical examination, CA-125 levels, and CT imaging.
• Intraperitoneal chemotherapy: Data suggest a substantial improvement in overall survival and progression-free survival in patients with newly diagnosed, optimally debulked stage III ovarian cancer by the administration of cisplatin and paclitaxel via an intraperitoneal (IP) port rather than the conventional intravenous (IV) administration. Studies have demonstrated an approximately 1-year increased survival with IP administration as compared to IV administration, although an increase in toxic events and catheter-related complications is a disadvantage of this therapeutic approach and may prevent completion of all six cycles.
• Alternative therapies including dose-dense (weekly) chemotherapy and biologic therapies are under investigation.
• Consolidation treatment: Eighty percent of patients who complete optimal tumor debulking followed by six cycles of carboplatin and paclitaxel will achieve a clinical remission. Consolidation treatment strategies to lengthen time to recurrence are currently being investigated. Prior studies using platinum and taxane agents for maintenance chemotherapy have not shown significant improvements in overall survival. Recent studies have demonstrated an improvement in progression-free survival when bevacizumab was administered along with IV carboplatin and paclitaxel and continued as a single agent for 10 months, although there was significantly no improvement in overall survival. Consideration of its use must reflect on its significantly increased cost without an improvement in overall survival. In patients with estrogen-positive primary tumors, hormonal therapies such as tamoxifen or aromatase inhibitors can also be considered.
P.635
Posttreatment Surveillance in Asymptomatic Patients
• Appropriate follow-up for asymptomatic patients after primary surgery and chemotherapy should include a physical examination with rectovaginal examination, CA-125 testing, and CT scan if clinically indicated. Patients should be seen every 3 months for the first 2 years, then every 6 months for the next 3 years.
• In patients whose CA-125 level was elevated preoperatively, CA-125 is a reliable marker of disease recurrence with a sensitivity of 62% to 94% and specificity of 91 % to 100%. Levels are often elevated 2 to 5 months prior to clinical detection of recurrence. However, a recent prospective randomized trial showed no difference in survival outcome for patients who were treated for recurrent ovarian cancer based on CA-125 level alone versus waiting for the development of symptomatic disease.
• CT scans have a sensitivity and specificity of 40% to 93% and 50% to 98% respectively for recurrent disease. One limitation is the poor sensitivity of detecting small volume disease. In a retrospective study, asymptomatic patients with recurrence detected by CT scan had a higher rate of optimal secondary cytoreductive surgery and improved overall survival compared to patients with symptomatic recurrence.
• Combined positron emission tomography imaging and CT may have clinical use in detecting disease recurrence in select patients and is often recommended prior to secondary cytoreduction.
• Second-look surgery by laparotomy or laparoscopy can be performed on patients with advanced epithelial ovarian cancer who have no clinical evidence of disease after undergoing primary debulking and adjuvant chemotherapy. The use of second-look surgery remains controversial and should be performed only in the setting of a clinical trial or on an individualized basis, as there are no data demonstrating improved survival with this approach. Patients need to be counseled that the procedure is not therapeutic but may provide prognostic information.
Recurrent or Persistent Disease
• Secondary debulking: Patients with recurrent or persistent disease may be candidates for further surgical therapy or secondary cytoreduction. Surgery should be reserved for patients in whom additional therapy has a good chance of prolonging life or palliating symptoms. The best candidates for secondary cytoreduction are those with longer disease-free intervals (at least 6 to 12 months) and fewer sites of recurrence.
• Second-line chemotherapy: Response rates for second-line chemotherapy are in the range of 20% to 40%. A host of chemotherapy options are available for recurrent ovarian cancer.
• Hormone therapy has been used as salvage treatment. Both megestrol acetate (Megace) and tamoxifen have been used to treat recurrent disease. Response rates are low.
• Radiation therapy is generally not used except for palliation of distant metastases.
• Experimental studies: Many investigators are currently studying the underlying molecular biology of epithelial ovarian cancer. Microarray analysis and proteomics provide insight into the differential expression of mRNA and proteins, respectively. Translational studies to further characterize these molecular changes, as they relate to the clinical disease state, provide an opportunity for novel therapeutic agents. Clinical trials are also currently investigating antiangiogenic drugs.
P.636
Complications of Advanced Ovarian Cancer
• Intestinal obstruction: Many women with ovarian cancer develop intestinal obstruction, either at initial diagnosis or with recurrent disease. Obstruction may be related to mechanical blockage or carcinomatous ileus. Correction of intestinal obstruction at initial treatment is usually possible; obstruction associated with recurrent disease, however, is a more complex problem. Some of these obstructions may be treated conservatively with IV hydration, total parenteral nutrition, and gastric decompression. The decision to proceed with palliative surgery must be based on the physical condition of the patient and her expected survival. If patients are unable to undergo surgery or are judged to be poor operative candidates, placement of a percutaneous gastric tube may offer some symptomatic relief. In cases of large bowel obstruction, the use of colorectal stents may be an option in order to avoid the significant morbidity and mortality associated with surgical management.
• Ascites: Initial ascites on presentation with ovarian cancer is almost always improved by debulking surgery and several courses of chemotherapy. Persistent ascites is difficult to manage and is a very poor prognostic sign. Ascites is best managed by serial paracenteses with fluid removal and chemotherapy.
Survival
• Age: Overall survival rate 5 years after diagnosis in women younger than age 65 years is nearly twice that of women older than age 65 years (57% and 28%, respectively).
• Stage: Patients with stage I disease have up to a 94% 5-year survival rate. In contrast, overall survival for women with distant disease on presentation is 29% (see T able 48-5).
• Performance status: The Karnofsky Performance Scale Index (Table 48-6) classifies patients according to their functional impairment and can be used to assess prognosis in individual patients. Lower scores are associated with worse survival for most serious illnesses.
Primary Peritoneal Carcinoma
• Primary malignant transformation of the peritoneum is termed primary peritoneal carcinoma, which clinically and pathologically resembles serous epithelial ovarian
P.637 cancer. Primary peritoneal carcinoma can therefore appear with a clinical presentation similar to ovarian cancer in patients with a history of oophorectomy or with pathologically normal-appearing or minimally involved ovaries. Extensive upper abdominal disease is common, and clinical course, management, and prognosis are similar to those for epithelial ovarian cancer.
TABLE 48-6 5-Year Survival for Epithelial Ovarian Cancer by Stage (2010)
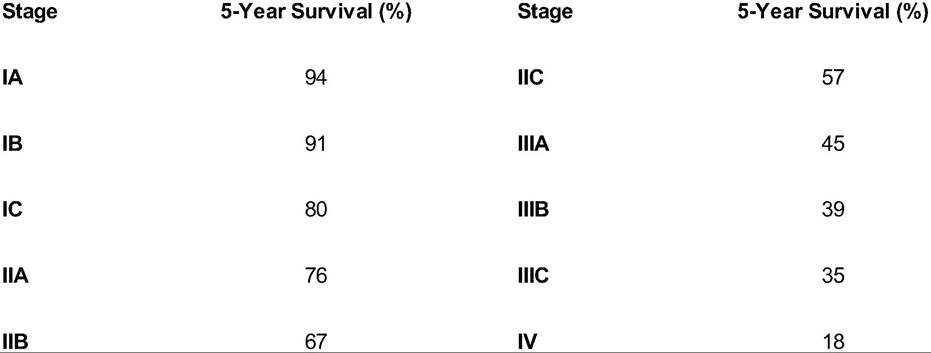
From American Cancer Society. Survival rates for ovarian cancer. American Cancer Society Web site. http://www.cancer.org/cancer/ovariancancer/overviewguide/ovarian-cancer-overview-survival. Accessed
September 20, 2010.
FALLOPIAN TUBE CANCER
• Epidemiology: Carcinoma of the fallopian tube is very rare, accounting for exist. Over 90% of tumors are papillary serous adenocarcinomas, resembling ovarian serous carcinomas.
• Clinical presentation and diagnosis: The triad of symptoms of fallopian tube carcinoma is watery vaginal discharge (hydrops tubae profluens), pelvic pain, and a pelvic mass. However, only 15% of patients present with this triad. Vaginal discharge or bleeding is the most common presenting symptom (50% to 60%), followed by abdominal pain and an abdominal mass. As in ovarian cancer, presentation may be nonspecific. Ascites may be present if the disease is advanced.
• Unlike ovarian cancer, fallopian tube carcinoma more often presents at an early stage. A preoperative diagnosis of fallopian tube cancer is made in only a minority of patients; the usual clinical diagnosis is ovarian tumor or pelvic inflammatory disease. The majority of patients will have elevated CA-125 levels.
• Natural history and patterns of spread: Tubal cancers spread in a similar fashion to ovarian cancers.
• Staging: Fallopian tube cancer is staged using the ovarian cancer staging system.
• Treatment is similar to that of ovarian cancer, with surgical debulking as the mainstay of treatment, followed by combination platinum-based chemotherapy. Chemotherapy for early-stage disease is the subject of controversy.
• Prognosis and survival are related to the stage of disease. Data on 5-year survival rates are as follows from stage I to IV: 95%, 75%, 69%, and 45%.
GERM CELL OVARIAN TUMORS
Epidemiology
• Approximately 20% of all ovarian tumors are of germ cell origin, with only 2% to 3% of these being malignant. Types include the following: dysgerminoma, endodermal sinus tumor, embryonal carcinoma, polyembryoma, choriocarcinoma, and teratoma.
• Roughly 70% to 80% of all germ cell tumors occur before age 20 years, and approximately one third of these are malignant. The median age of women diagnosed
P.638 with a malignant germ cell tumor is 16 to 20 years. About 50% to 75% of patients with malignant germ cell tumors present with stage I disease. Overall survival rates, including those with advanced disease, are 60% to 80%.
• The most common germ cell tumor is a benign cystic teratoma (dermoid), and the most common malignant tumor is the dysgerminoma.
Pathology
• Germ cell tumors are derived from the primordial germ cells of the ovary; however, they are a heterogeneous group of tumors. They gradually differentiate to mimic tissues of embryonic origin (ectoderm, mesoderm, endoderm) and extraembryonic origin (trophoblast, yolk sac). They are aggressive tumors, frequently unilateral, and usually curable if treated early.
Diagnosis
• Clinically, germ cell malignancies grow quickly and are often characterized by acute pelvic pain. The pain can be caused by distention of the ovarian capsule, hemorrhage, necrosis, or torsion. A palpable pelvic mass is a common finding on presentation. Abdominal distention and abnormal vaginal bleeding may also be the presenting complaint. The tumors are often large at presentation, with a median diameter of 16 cm.
• Ovarian masses that are 2 cm or larger in premenarchal girls or >8 to 10 cm in premenopausal patients generally require exploratory surgery.
• Preoperative workup: Measurement of serum tumor markers may assist in the diagnosis of germ cell malignancies (Table 48-7). Workup should include measurement of serum human chorionic gonadotropin (hCG), alpha-fetoprotein (AFP) titers, lactate dehydrogenase (LDH) levels, a complete blood count, and liver
P.639 function tests. A chest radiographic study is important to rule out pulmonary metastases. A preoperative CT scan should be considered to assess for the presence or absence of liver metastases and retroperitoneal lymphadenopathy.
TABLE 48-7 The Karnofsky Performance Scale
Description %
Normal; no complaints; no evidence of disease 100
Able to carry on normal activity; minor signs and symptoms of disease 90
Normal activity with effort; some signs and symptoms of disease 80
Cares for self; unable to carry on normal activity or do work 70
Requires occasional assistance but is able to care for most personal needs 60
Requires considerable assistance and frequent medical care 50
Disabled; requires special care and assistance 40
Severely disabled; hospitalization indicated although death not imminent 30
Very sick; hospitalization necessary; requires active support treatment 20
Moribund; fatal processes progressing rapidly 10
Dead 0
Originally published by Karnofsky DA, Burchenal JH. The clinical evaluation of chemotherapeutic agents
in cancer. In Macleod CM, ed. Evaluation of Chemotherapeutic Agents. New York, NY: Columbia University, 1949:199-205.
Germ Cell T umor Types
• Dysgerminomas are the most common malignant germ cell tumor, comprising up to 50%. All dysgerminomas are malignant; however, not all are aggressive. Seventy-five percent of dysgerminomas occur in the second and third decades of life. They are the only germ cell tumor that tends to be bilateral (10% to 15% of cases). The 5-year survival rate for stage IA disease is 95% and for all stages is 85%.
• Endodermal sinus tumors (yolk sac tumors) are derived from cells of the primitive yolk sac and are the second most common malignant germ cell tumor, accounting for 20% of cases.
• Histologically, they are characterized by Schiller-Duval bodies. These tumors tend to grow rapidly and aggressively. They secrete AFP. The disease-free survival for all stages is >80%.
• Embryonal carcinoma tumors are extremely rare and occur in children and young adults. They may secrete both hCG and AFP. Patients may present with sexual precocity and vaginal bleeding.
• Polyembryoma tumors are exceedingly rare and highly malignant. They resemble early embryos and may secrete AFP or hCG.
• Nongestational choriocarcinoma: Pure, nongestational choriocarcinoma involving the ovary is very rare and is histologically similar to gestational choriocarcinoma (see Chapter 49). Almost all patients are premenarchal. This tumor often produces remarkably high levels of hCG, which may in turn increase thyroid function. Precocious puberty is seen occasionally, and patients may present with vaginal bleeding. Historically, choriocarcinomas have had a poor prognosis but tend to respond to combination chemotherapy.
• Immature malignant teratomas contain tissues resembling those in an embryo. They account for 20% of malignant germ cell tumors and 1% of ovarian malignancies. Half of immature teratomas occur in patients between ages 10 and 20 years. These tumors may secrete AFP. The most important prognostic factor is tumor grade. The 5year survival rate is 95% for stage I disease and 75% for advanced disease.
• Mixed germ cell tumors account for 10% of malignant germ cell tumors and contain elements of two or more of the germ cell tumors discussed previously.
Management of Germ Cell T umors
• Surgical: Primary treatment for all germ cell tumors is surgical and should include proper surgical staging to rule out the presence of extraovarian microscopic disease. Because most patients are of reproductive age, preservation of fertility is important.
• Unilateral oophorectomy is performed along with unilateral pelvic and para-aortic lymphadenectomy. A frozen section should be obtained. Bilateral involvement is rare in germ cell tumors, with the exception of dysgerminomas (10% to 15% bilaterality).
• The contralateral ovary should be inspected, and a biopsy may be performed if there is suspicion of involvement. The ovary should only be removed in a young patient if disease is present. The remaining pelvic organs may be left in situ to preserve fertility.
• For patients who have completed childbearing, a total abdominal hysterectomy with bilateral salpingo- oophorectomy is reasonable. If metastatic disease is present on initial surgery, cytoreductive surgery is recommended, although data are limited.
TABLE 48-8 Serum Markers for Germ Cell and Sex Cord-Stromal Ovarian Tumors
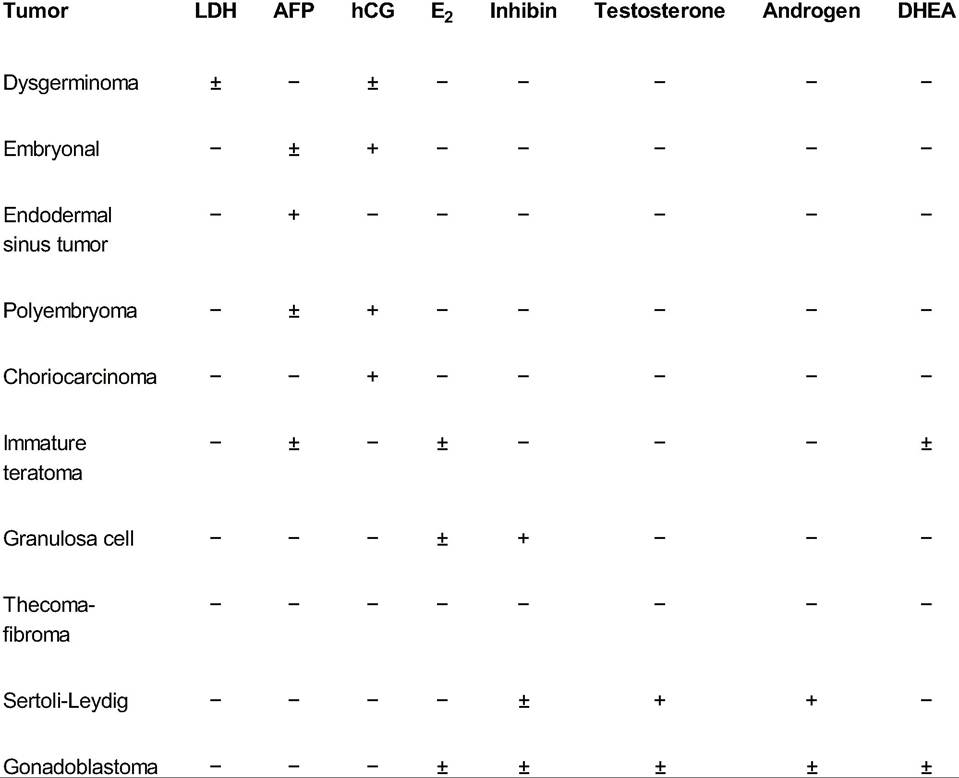
LDH, lactate dehydrogenase; AFP, alpha-fetoprotein; hCG, human chorionic gonadotropin; E2, estradiol; DHEA, dehydroepiandrosterone.
• Surgical therapy alone is recommended for stage IA dysgerminomas and stage IA, grade I immature teratomas. These patients have a 5-year survival of >90%. Approximately 15% to 25% will recur but can be treated successfully at the time of presentation. For endodermal sinus tumors, staging is not always recommended because chemotherapy should be given regardless.
• Adjuvant therapy: The decision to administer adjuvant therapy depends on the histologic type of germ cell tumor. Except those with stage IA, grade I immature teratoma and stage IA dysgerminoma, all patients require postoperative chemotherapy. Dysgerminomas are very sensitive to radiation therapy; however, fertility is lost as a consequence of irradiation. Therefore, chemotherapy is the first-line treatment. Combination therapy with three agents (bleomycin, etoposide, and cisplatin [BEP]) is recommended, although in some cases, bleomycin may be omitted due to its significant pulmonary toxicity. Prognosis has significantly improved with platinumbased chemotherapy.
• Ninety percent of patients with germ cell tumors who experience a recurrence will do so in the first 2 years after therapy. If initially treated with surgery alone, BEP chemotherapy can be used. Patients who initially received chemotherapy can be treated with a platinum-based agent.
SEX CORD-STROMAL OVARIAN TUMORS
Sex cord-stromal tumors are derived from the sex cords and mesenchyme of the embryonic gonad and account for 5% to 8% of all ovarian neoplasms (Table 48-8). Most of these tumors are hormonally active. Types include the following: granulosa-stromal cell, Sertoli-Leydig, sex cord tumor, and gynandroblastoma.
P.641
Granulosa Cell T umor
• Incidence: The granulosa cell tumor is the most common malignant sex cord-stromal tumor, accounting for 70% of cases. Adult granulosa cell tumors occur primarily in the perimenopausal years, with a mean age of 52 years at presentation. Two forms exist: an adult form (95%) and a much rarer juvenile form (5%). The tumor is bilateral in 10 cm in diameter. Granulosa cell tumors are characteristically hemorrhagic and can present with a hemoperitoneum.
• The incidence of concurrent endometrial hyperplasia is over 50%, and the incidence of concurrent endometrial adenocarcinoma ranges from 3% to 27%, demonstrating the importance of endometrial biopsy when the diagnosis of granulosa cell tumor is made. The majority (90%) of affected patients present with stage I disease, mainly because the hormonal effects of the tumor cause symptoms early in the disease. In juvenile type, patients present with pseudoprecocious puberty and have elevated serum estradiol.
• Treatment: Surgery alone is usually sufficient treatment only for stage IA or IB disease. For all other stages, platinum-based chemotherapy is recommended. Carboplatin and paclitaxel has been increasingly used; however, regimens used for germ cell tumors (BEP) can also be considered. Radiation and/or chemotherapy can be used to treat recurrent disease. If the patient desires to maintain fertility, a unilateral salpingo-oophorectomy is adequate for treating stage IA tumors, and surgical staging should also be performed. With completion of childbearing, a total abdominal hysterectomy and bilateral salpingo-oophorectomy should be performed. If the uterus is left in situ, the patient should undergo dilation and curettage to rule out endometrial hyperplasia or adenocarcinoma. Chemotherapy after surgery has not been shown to reduce the recurrence risk.
• Prognosis and survival: Granulosa cell tumors have a propensity for late recurrence, which has been reported as long as 30 years after treatment of the primary tumor. The 10-year and 20-year survival rates are 90% and 75%, respectively.
Sertoli-Leydig Cell T umor
• Incidence: Sertoli-Leydig cell tumors account for only 0.2% of ovarian neoplasms. The average age at diagnosis is 25 years. These tumors are most frequently low-grade malignancies, and nearly all patients (97%) present with stage I disease.
• Diagnosis and presentation: Sertoli-Leydig cell tumors often produce androgens. Patients present with virilization (30% to 50%), menstrual disorders, and symptoms related to an abdominal mass. The average size of these tumors is about 16 cm. They may produce testosterone, androstenedione, or AFP.
• Treatment: In young patients, unilateral salpingo-oophorectomy with staging may be performed to preserve fertility. In older patients, a total abdominal hysterectomy and bilateral salpingo-oophorectomy should be performed as well. T reatment of those with higher stage and/or grade typically includes chemotherapy.
• Prognosis and survival: Prognosis is related to stage and histologic grade. The 5-year survival rate is 70% to 90%.
SPECIAL CONSIDERATIONS IN OVARIAN CANCER
• Metastatic tumors account for 5% to 20% of ovarian malignancies and are often, but not always, bilateral.
• Gastrointestinal tract tumors are the most likely to metastasize to the ovary. Krukenberg tumors of the stomach are usually bilateral and account for 30% to 40% of metastatic tumors to the ovary. These tumors are characterized histologically by signet ring cells, in which the nucleus is flattened against the cell wall by the accumulation of cytoplasmic mucin. In postmenopausal women who undergo evaluation for an adnexal mass, metastatic colon cancer should be ruled out, using colonoscopy if possible.
• Breast cancer is the second most likely cancer to metastasize to the ovary.
• Lymphomas can also metastasize to the ovary. Burkitt lymphoma may affect children or young adults. Rarely, ovarian lesions are the primary manifestation of disease in lymphoma patients.
• Metastatic gynecologic tumors may involve the ovaries. Fallopian tube cancer is the most common malignancy to metastasize to the ovaries and occurs by direct extension. Cervical cancer very rarely spreads to the ovaries without other sites of metastasis. Endometrial cancer may metastasize to the ovaries; however, synchronous endometrioid adenocarcinoma, primary to both the ovary and the endometrium, can also occur.
• Ovarian carcinosarcomas, also known as malignant mixed mesodermal tumors of the ovary, are extremely rare. These lesions are very aggressive, and treatment consists of surgical resection followed by combination chemotherapy. They are associated with a low response to treatment and overall poor outcome.
• Ovarian tumors during pregnancy are very rare. The incidence of an adnexal mass during pregnancy is approximately 1 in 800. The majority of adnexal masses discovered during the first trimester resolve by the second trimester. However, approximately 1% to 6% of these masses are malignant.
• Germ cell tumors (primarily dysgerminoma) account for approximately 45% of ovarian malignancies diagnosed in pregnancy.
• Masses are usually diagnosed during routine ultrasonography or at the time of cesarean section. The majority of patients (74%) are diagnosed with stage I disease.
• Early-stage disease can be treated with conservative surgery in the second trimester of pregnancy, usually with good maternal and fetal outcomes. Late-stage and high-grade disease should be treated aggressively after appropriate counseling of the patient.
SUGGESTED READINGS
Armstrong DK, Bundy B, Wenzel L, et al; Gynecologic Oncology Group. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006;354:34-43.
Burger RA, Brady MF, Bookman MA, et al; Gynecologic Oncology Group. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med 2011 ;365:2473-2483.
Hoskins WJ, Perez CA, Young RC, eds. Principles and Practice of Gynecologic Oncology, 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2005.
Kauff ND, Domchek SM, Friebel TM, et al. Risk-reducing salpingo-oophorectomy for the prevention of BRCA1- and BRCA2-associated breast and gynecologic cancer: a multicenter, prospective study. J Clin Oncol 2008;26(8):1331-1337.
Kurman RJ, Shih IeM. The origin and pathogenesis of epithelial ovarian cancer—a proposed unifying theory. Am J Surg Pathol 2010 34(3):433-443.
Vergote I, T rope CG, Amant F, et al; European Organization for Research and T reatment of Cancer- Gynaecological Cancer Group; NCIC Clinical Trials Group. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med 2010;363(10):943-953.