Managing uncertainty vs. managing death
HIV disease constantly challenged the acute/palliative interface with clinical constellations in which “curable” and palliative elements coexist. HAART (highly activated antiretroviral therapy) is the most recent example since which progression beyond “treatability” is less easy to discern.
Similarly in cancer, palliative care's role now includes support early in the disease journey to help manage the uncertainties associated with toxic treatments as well as the worries about disability and mortality. Such psycho-emotional, spiritual and social fallout is beyond the capabilities of linear, curative medicine to manage. Palliative (symptom-based) and therapeutic (pathology-based) approaches are not mutually exclusive. The unifying concept of palliative care these days is the management of uncertainty and suffering, only part of which is care of the dying.A challenging disease
Many patients with HIV/AIDS come from marginalised groups. Characteristically, these minorities take up services late or sit uneasily with conventional care because of different health beliefs or mistrust. Consequently, we cannot approach them all in the same way; neither can we assume what makes a good death nor what comprises a family or close social group. These are the practical realities of patient-centred care.
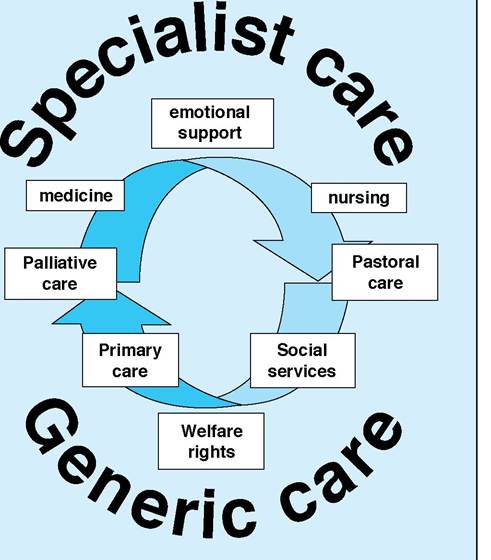
Figure 14.1 Inter- and multidisciplinary care: essential professional groupings necessary for effective supportive and palliative care
Flexibility, collaboration and support
Effective care for patients in whom deterioration or death is a real but fluctuating possibility also confronts us with the need to integrate care flexibly. Patients facing chronic ill health or those with acute, highly symptomatic disease may benefit from specialist advice or shared care as much as those may in the terminal phase of their illness.
It is only by close collaboration between teams that good outcomes will be achieved. This brings us to our shared problem: that of uncertainty and the ways in which curative and palliative strategies coexist.The therapeutic dilemma
When palliation is simply supporting aggressive curative therapy, there is no problem. However, when disease is progressive or debilitating, or where prophylactic and maintenance regimens maintain residual health, but compromise the quality of the patient's life, therapeutic decisions must take account of the burdens and benefits in personal as well as pathological terms. This is the idea that treatments may be futile not just by being ineffective, but also by being so destructive to quality of life that they may be worse than useless. Ethicists call this qualitative futility. In order for us to be of genuine benefit clinically, we must find effective ways of living in this tension between cost and benefit.
The quantity/quality equation
Balancing the costs and benefits of treatment formally and explicitly clarifies a patient's best interest, particularly as health
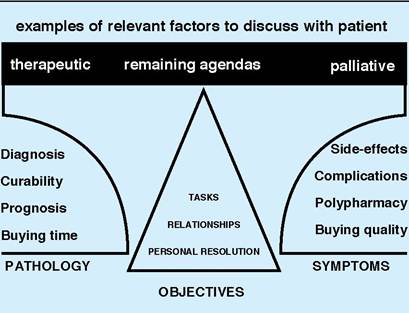
Figure 14.2 Treatment — applying a cost-benefit ratio
begins to fail. Certainties, such as time and energy expended on a course of treatment or immediate and short-term benefits etc. then become increasingly important.
Try not to make assumptions about a patient's views or wishes. The subtle ways in which illness and the individual interact mean that social, psychological and existential/spiritual elements may be every bit as relevant to symptomatology as the underlying pathology. Be sure to discuss these issues with the patient trusting that those not wanting to be involved in decision-making will let you know. Refer on for psychological or pastoral help if you need to.
Working with uncertainty
One of the greatest fears for the chronically sick or dying is helplessness.
The more a patient and family feel their agendas, wishes and hopes are being taken seriously, the better able they are to cope.Never make rash promises or be blindly optimistic about all treatments. Patients respond very negatively to hopes that are raised and dashed. Professional denial is the single most common cause of anger expressed by patients against doctors. Avoid presenting options as unchallengeable. There are ways to communicate boundaries or margins of our uncertainty to ensure that patients are informed. Don't forget, consent is a dynamic process.
Discussing prognosis
Open sharing of information inevitably leads to questions about prognosis. Always speak to individuals where they are able to express emotions openly. Never do it on an open ward. Include significant others if possible and invite another professional (for example, the key nurse), who can reinforce the discussion and offer support after you have gone. Patients and families need to “re-run” many times and characteristically will hear only the first and last thing that you say.
To gauge a patient's level of knowledge, anxiety or fear, explore their understanding of the situation by starting conversations in an open way, simply by asking what they think is going on or how they feel their disease is fairing.
When you talk about time, according to the stage of illness, break the future into tangible and appropriately small blocks of time such as one to three months. The intervals chosen will depend on each case. Confine your prognostication to this period and use general terms such as better, the same or worse.
Never give a finite prognosis. Always say that the unexpected may happen. If possible arrange to review the discussion to answer outstanding questions. This will also provide the opportunity to revise an opinion.
Summary
Palliative and curative care are inescapably entwined but changeable and good practice recognises the fluid involvement of different colleagues in care.
Palliative care brings: ways of talking about and engaging uncertainty, looking at care planning and dealing with the ethical difficulties around consent and refusals and is valuable at any stage of illness. Palliative care workers should be called on when necessary, not just when you have run out of options and certainly not left until a patient is actually dying.Box 14.1 The essentials of partnership with patients
• The patient’s priorities may be very different from yours
• Try not to make assumptions about a patient’s views or wishes
• Quality of life generally, but not necessarily, becomes more important than the quantity as health wanes
• Be sure to discuss costs and benefits openly and in detail
Box 14.2 The patient is at the centre of decisionmaking
• Work in partnership with the patient and family
• Share responsibility for making decisions
• Maximise the patient’s control over decision-making
• Work in a positive framework
• Agree specific tasks
• Set realistic goals
• Review regularly
• Remain open to creative options
Box 14.3 Consent is a dynamic process
• Set goals and objectives with the patient.
• Revised them as regularly as necessary — clearly it would be stupid to review weekly when a patient’s prognosis is years and equally unhelpful to give a patient a 2-month appointment when you expect them to die in a few weeks.
• Particularly, review aggressive treatment to reach a specific goal immediately that objective is met: a patient’s wishes may alter radically as a result of success or failure.
• Be realistic, yet at the same time be prepared to allow a patient to risk things such as travel, provided they are well informed.
• Above all plan positively: people wish to live not to exist.
Box 14.4 Answering questions about prognosis
• Choose a “safe” place
• Include significant others and/or other professionals
• Explore the patient’s understanding
• Be honest; don’t collude with unrealistic hopes and don’t be afraid to say “I don’t know”
• Be kind; allow the patient to set the limits on the discussion when exploring painful truths
• Arrange a future contact