Faecal incontinence
Definition
Faecal incontinence is the involuntary loss of control of a person’s bowels. It can affect over 10% of adults and at least 1-2% of patents will report these as major symptoms.
In itself, faecal incontinence is not a disease but a symptom and it is necessary to take a full history and examine a patient to identify any underlying diseases or pathology that may need treatment before focusing on managing incontinence.The majority of causes of faecal incontinence are acquired. The congenital causes are rare and include imperforate anus, rectal agenesis, and cloacal defects as well as spina bifida. Acquired causes can be divided into anorectal causes—anatomical disruption, neurological causes and age-related causes, or colonic and metabolic causes.
The aim of any treatment for faecal incontinence is to improve the patient’s quality of life and give them some control back over their bowel function.
There are three main types of faecal incontinence:
• Urge incontinence—when the arrival of stool in the rectum is associated with a rise in rectal pressure and the external anal sphincter is unable to squeeze shut sufficiently to prevent the forcing of the stool out through the anal canal.
• The second type of incontinence is passive incontinence. This is usually due to internal sphincter dysfunction which either occurs by direct damage to the muscle or through poor function. This results in symptoms of leakage—the patient is usually unaware of faecal loss until their pad or underwear is stained. It can occur at any time of the day and may be associated with exercise.
• The third type of incontinence is post-defecatory leakage. This is when a patient has gone to the toilet, emptied their bowels, and then within the next half hour finds that they have leaked under their underwear. It is often associated with difficulty in cleaning.
The aetiology of this is often a rectocele or haemorrhoids and it may be associated with poor rectal emptying; these anatomical problems can be more relatively easily treated.History and examination
It is essential that anybody presenting with new onset of incontinence has a full history of bowel symptoms taken. This is particularly looking for any of the ‘red flag’ symptoms associated with bowel cancer. These are change in bowel habit to looser stools and rectal bleeding. Patients with these symptoms should be referred for further investigations. The person presenting with incontinence should be able to describe when the incontinence happens, whether it is associated with the need to go to the toilet (urge incontinence), whether it is associated with walking, whether it happens at a random time (passive incontinence), and the consistency of the motions involved. Incontinence to wind is often a significant issue and may be associated with certain dietary habits. A medication review is essential as certain drugs, for example, metformin, are associated with loosening of the stools and further incontinence.
Examination should include an abdominal examination as well as a visual inspection of the perineum looking for signs of previous episiotomy or tears. A gaping anus will suggest a poor internal anal sphincter. Any anorectal pathology such as fistula or fourth-degree piles should be noted and the patient should be asked to strain to see how much descent of pelvic floor occurs. At the time of straining, assessment of a rectocele and cystocele can be made and this is often easier if the patient is in the lithotomy position in a gynaecological chair. Rectal examination allows the doctor to exclude faecal impaction and overflow and to assess both anal tone and squeeze pressure. It is also useful to be able to place a finger towards the vagina to see whether there is a rectocele and whether the patient has a similar sensation of pocketing as when the finger is placed within the rectocele.
Measuring faecal incontinence
Quantifying the degree of faecal incontinence is important to assess the outcomes of various treatment options. Faecal incontinence can be to solid, liquid, or gas and the impact on quality of life can vary greatly between patients. The Wexner (or Cleveland Clinic) score (Figure 58.5) is widely used and scores five domains from 0 to 4 (giving a maximum score of 20). It is generally considered that a score of 9 or more is considered to represent significant incontinence.
The Faecal Incontinence Quality of life questionnaire has 29 items and has good correlation with psychometric evaluation of symptom impact; it is more complicated and time-consuming to complete.
Treatment
Initial bowel management
Many patients with incontinence can be treated with simple aids. Dietary modification to reduce the volume of stool and the softness of the stool can be particularly helpful. There have been two studies which showed considerable impact by lifestyle change on
Cleveland Clinic incontinence score
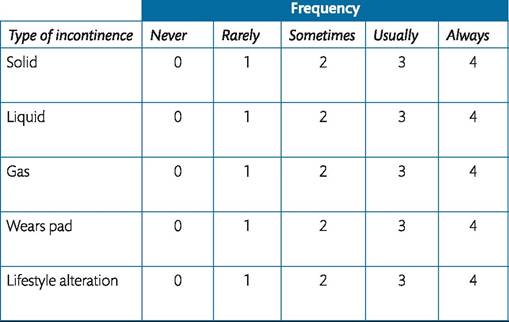
Never, O; rarely, <1∕month; sometimes, <1∕week, ?≈1 /month; usually, <1∕day, ?≈1∕week; always, ?≈1∕day.
O, perfect; 20, complete incontinence.
Figure 58.5 Cleveland Clinic incontinence score. anal incontinence. The first by Bliss et al. (8) showed that a selfcare change of diet or avoidance of certain foods were successful in helping 67% of an elderly mixed cohort of patients presenting with anal incontinence reduce their symptoms. The second study from 2010 (9) showed that lifestyle changes can improve anal incontinence in about a third of the general population.
The most important things within the diet to change are those that result in loose or softer stools; these are foods that contain wheat fibre, pulses, beans, caffeine, and also lactose-containing food.
There are a variety of continence aids that will help patients with faecal incontinence and the newer ones of these are anal plugs. There are two plugs that are available on the National Health Service (NHS) in the United Kingdom. There is, however, little in the way of evidence that these will work except in highly motivated patients. The studies that are published on plugs are relatively poor in terms of methodology. They have limited follow-up and the dropout rates are high. However, continence can be achieved in highly motivated patients with good compliance in up to 37% of people (10, 11).
Medication
One of the mainstays of treatment of faecal incontinence is the use of medication. There are three widely used drugs that control soft or looser stools. Loperamide, a synthetic opioid that does not cross the blood-brain barrier, is the commonest one to be used for faecal incontinence. It has an excellent safety profile and acts directly on the intestine to inhibit peristalsis increasing small intestinal and mouth-t o-caecum transit time; this allows more water to be absorbed from the stool. There is some evidence that loperamide may act directly on sphincter tone and resting pressure and may increase rectal perception in healthy subjects. An alternative drug is codeine phosphate, which acts in a similar way to loperamide but crosses the blood-brain barrier and therefore may cause dependency. Finally, Lomotil (diphenoxylate and atropine) is occasionally used; it also crosses the blood-brain barrier and is therefore usually used with a low dose of atropine to prevent over usage. Omar and Alexander published a Cochrane review of medical treatment in 2013 (12). This study identified 16 trials and included 558 participants. There was some limited evidence that antidiarrhoeal drugs may reduce faecal incontinence in patients with liquid stools. The side effects of loperamide such as constipation, abdominal pain, diarrhoea, headache, and nausea were greater than in the placebo group.
A liquid form of loperamide (Imodium, paediatric) is available and is widely used by clinicians; it allows titration of symptoms with accuracy to try and reduce volume of stool and minimize side effects. Many patients find this a useful treatment.Exercises and biofeedback
One of the mainstays of further treatment is pelvic floor exercises, bowel training, and biofeedback. Biofeedback relies on strength training, rectal sensitivity training, and improving coordination of the rectum and anus. In a randomized controlled trial from St Mark's Hospital, Harrow, United Kingdom (13), 171 patients were randomized to four groups. All four groups received patient teaching, emotional support, lifestyle modification, and a programme to explain how to manage both faecal incontinence and urge incontinence. The second group received additional anal sphincter exercises with 50 squeezes a day. The third group had clinic computer biofeedback and the fourth group had in addition to all of these a home biofeedback unit. The results showed that there was no significant difference between the groups; however, all groups had a 50% improvement and the episodes of incontinence throughout the groups reduced from a median of 2 to 0. The incontinence score decreased from 11 to 8.
There are different styles of biofeedback and exercise regimens from sustained squeeze manoeuvres to rapid squeeze manoeuvres and no significant difference has been shown between these different methods. However, what these patients do show is a prolonged improvement in general by having intervention by medical and nursing teams. The Cochrane review from 2012 looking at biofeedback and sphincter exercises reviewed 1525 participants. This suggested that there was not enough evidence to show that any particular method of biofeedback or exercises was better than any other. However, many patients will improve with some form of intervention. The final non-medical way of treating incontinence is to use some form of emptying device.
This can be glycerine suppositories, enemas, or water-based systems and many of these are available on the market.Surgical treatment
There have been a variety of surgical approaches to repair or replace anal sphincters in order to treat faecal incontinence.
Overlapping sphincter repair/sphincteroplasty
For many years the only treatment available for sphincter disruption was an overlapping anterior sphincter repair (Figure 58.6). This is done not at the time of the original injury, which usually falls under the remit of the obstetrician, but sometime later after either an occult injury is diagnosed or symptoms have deteriorated from previous surgery. In 2012, the long-term outcomes of the many series within the literature were reviewed (14). The majority of series had mostly obstetric injury patients and the number of patients involved varied from 14 to 191 within each series. The length of follow-up was anything from 5 to 10 years and the results were classified as either excellent or good, fair, or poor. Fair represented minimal improvement or no change whereas poor outcomes included worsening incontinence. Although there was considerable variation across the studies, in the majority the long-term results were that approximately 50% maintained good or excellent results but 50% had fair or poor results. Most of the studies found that there was a poorer outcome with wound infection and older age.
Artificial bowel sphincter
In 1987, John Christenson suggested using the urinary sphincter as an artificial bowel sphincter and over 500 cases have been implanted worldwide. The National Institute for Health and Care Excellence (NICE) reviewed the use of artificial bowel sphincters and suggested that they may still have a place in patients with significant sphincter disruption or following failure of sacral nerve stimulator and sphincter repair. The Cochrane review in 2010 suggested that the artificial bowel sphincter may be better than conservative treatment but has significant morbidity. This morbidity has been well documented by Paul Lehurs unit in Nantes (15) where in 52 patients followed up for a mean of 5 years over a quarter had their devices explanted due to infection and there was a high rate of revision with over 50% of patients needing some form of revision.
Dynamic graciloplasty
The transposition of the gracilis muscle to reconstruct the anus was first described in 1952 (16); this had relatively poor results and it was not until 1991 when a stimulated dynamic graciloplasty was reported that the procedure started to be adopted by colorectal surgeons (17, 18).
This is an invasive surgical procedure and is reserved for patients who have failed conservative management and do not have a repairable sphincter defect. The procedure involves mobilizing the gracilis muscle, either unilaterally or bilaterally, and wrapping it around the anus, attaching it to the contralateral ischial tuberosity. These procedures are associated with considerable morbidity and mortality and in a small series of 38 patients (19) with a median follow-up of 5 years there were 13 infections and 2 immediate gracilis problems in the short term. In the long-term, 10 patients required 15 procedures to replace pacemaker components and 24 patients suffered from some morbidity in the donor leg including pain, swelling, and paraesthesia. After long-term follow up, 30% had a stoma and although 22 still had a functioning graciloplasty, 13 were incontinent daily, 11 required some form of enema or irrigation to empty, and 64% still had bowel function that adversely affected their daily lives. In view of this, NICE suggested that this procedure was only supported in specialist units and indeed it is no longer available in the United States.
Fenix procedure
A newer procedure to encircle the anal sphincter with titanium wire and magnetic beads has more recently come into practice. It is relatively easily placed in a tunnel in the ischioanal fossa just beneath the levator ani and the number of beads can be measured to fit for each individual patient. The first 35 patients having a Fenix were published in the literature (20). These patients showed an improvement in their Cleveland Clinic Score from 16 to an average of 7.3 with significant improvement in faecal quality of life. There were no intraoperative complications in this series, there were, however, three infections, one device separation problem, two patients had a stoma because of lack of efficacy of the procedure, and one patient had transvaginal erosion.
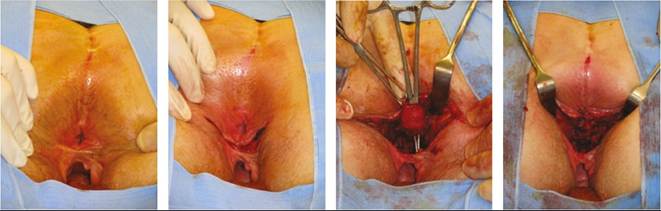
Figure 58.6 Overlapping sphincter repair.
Other sphincter augmentation methods
Some centres are treating patients with the SECCA system. This is radiofrequency energy delivered to the anal canal that is said to remodel and tighten the collagen. It is done at three to four levels through the anus and some short-term results have suggested an improvement in patients’ incontinence scores. However, this is not covered in the NHS and should only be performed in a trial situation.
Anal bulking agents
Over many years surgeons have tried to inject a variety of molecules into the internal anal sphincter or the anal cushions to improve passive leakage by recreating the anal seal. Back in 1993, Teflon was used followed by autologous fat, collagen, silicone, carbon-coated beads, and more recently porcine collagen and hyaluronic acid. Many of these injectables have been associated with complications of granulomas, emboli, and migration of the molecules as well as infection. The studies that have been published show low numbers of patients with short length of follow-up and relatively little improvement in symptoms or incontinence scores. The NICE guidelines from February 2007 suggested that these procedures should only be used in units specializing in assessment and treatment of faecal incontinence and could only be done within a trial or audit.
Sacral neuromodulation
Sacral nerve stimulation (SNS) as a procedure has transformed the treatment of severe faecal incontinence. This was initially described for the treatment of urinary incontinence in 1981 and subsequently for faecal incontinence in 1995. It is now a well-accepted treatment for faecal incontinence for patients with or without a sphincter defect with both good short- and long-t erm results. Patients are assessed with a bowel diary (Figure 58.2) and should be incontinent at least two or three times a week in order to be considered for sacral neuromodulation. The patients complete a bowel diary before intervention but after maximum medical therapy, physiotherapy, and biofeedback and then have a temporary wire placed through the sacrum onto S3 or S4, usually S3 (Figure 58.7). If there is a greater than 50% improvement in symptoms, the patient then has a permanent wire placed into the sacrum and attached to a pacemaker battery which is buried in the ipsilateral buttock.
The mechanism of action remains unclear. It is hypothesized that the impulses modulate autonomic and somatic afferent and efferent impulses from the anus and rectum, thereby improving rectal compliance and increasing anal resting pressure (21).
A recent meta-analysis (22) looked at studies published between 1995 and 2008 on SNS for faecal incontinence. Thirty-four studies were included, reporting on 944 patients undergoing peripheral nerve evaluation; 665 then underwent conversion to a permanent SNS. Weekly incontinence episodes and incontinence scores were significantly improved (P <0.001). Results were similar between sphincter intact and impaired subgroups. The complication rate was 15% for permanent SNS, with 3% resulting in permanent explantation.
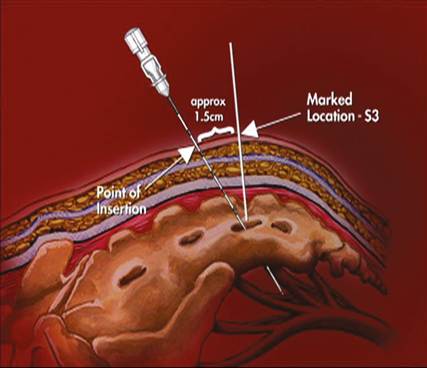
Figure 58.7 Sacral nerve stimulator landmarks.
Posterior tibial nerve stimulation
Peripheral neuromodulation was first described as a method of treating faecal incontinence by Shafik in 2003 (23). As with SNS, the mechanism remains unclear. It is thought that stimulation of the posterior tibial nerve at the ankle may send retrograde stimulation to the sacral nerve. A recent randomized multicentre study investigating posterior tibial nerve stimulation versus sham in patients with faecal incontinence found that 38% of patients in the treatment group and 31% of patients in the sham stimulation group reported a greater than 50% improvement in the number of incontinence episodes (24). This was not significantly different and the treatment is undergoing further evaluation.
End colostomy
This is a disfiguring operation with a significant long-term complication rate. It is reserved for patients who have failed other therapies or for those who are fully informed and understand the implication of long-term stomas. The formation of a stoma is not a specialized procedure and can be performed in a local hospital. However, the patients should be warned that up to a third of patients having these made for incontinence may experience significant issues with leakage from the rectal stump.
Summary
Faecal incontinence has many causes. An accurate history and examination is required to eliminate pathology that requires treatment (e.g. cancer). Simple dietary and lifestyle changes along with medication and exercises may improve patients’ quality of life in at least 50% of patients. Those with continuing symptoms should be investigated with anorectal physiology and ultrasound and be examined by a clinician with an understanding of all treatment options available. Patients with a cloacal deformity and/or large sphincter defect may be offered an overlapping sphincter repair. Sacral neuromodulation shows lasting good results in the 75% who show significant improvement with temporary stimulation. There is still a role for an end colostomy in patients with significant faecal incontinence refractory to all other measures.