Constipation and obstructive defecation
Definition
Constipation is an increasing problem in the Western world and it is widely accepted that approximately 50% of adults are constipated at any point in time. Constipation encompasses a multitude of symptoms; the general mental health and social functioning of people with constipation is impaired when compared to health controls.
Constipation can mean many things to many people. However, there are well defined criteria such as the Rome II criteria which allow us to compare patients' symptoms and treatment results. The Rome II criteria suggest that constipation can be diagnosed if two or more of the following symptoms have occurred for at least 12 weeks, not necessarily consecutively in the preceding 12 months. Symptoms include straining during more than 25% of bowel movements; lumpy or hard stools for more than 25% of bowel movements; a sensation of incomplete evacuation for more than 25% of bowel movements; a sensation of anorectal blockage for than 25% of bowel movements; and/or the need to use manual manoeuvres to aid defecation for more than 25% of bowel movements. These symptoms along with less than three bowel movements per week result in a diagnosis of constipation.Constipation can then be categorized into three different types: slow transit constipation, normal transit constipation, and obstructive defecation. Obstructive defecation or difficulty in evacuation is often associated with both normal transit and slow transit constipation.
Prior to a diagnosis of constipation other potential metabolic or physical causes for constipation should be excluded. These include carcinoma or pathology within the colon. Blood tests should be performed to exclude hypothyroidism, hypercalcaemia, and diabetes, all of which may be associated with constipation. A variety of neurological diseases including Parkinson's disease and multiple sclerosis are also associated with constipation.
Once a complete history has been taken, a physical examination has been made, and significant organic pathology has been excluded, there are three main other tests that can be done to evaluate constipation further: colonic transit studies, proctography, and anorectal physiology.
Treatment for constipation
The mainstay of treatment of constipation is use of a variety of laxatives, all of which have different modes of action. There is some evidence that increased physical activity is associated with less constipation and that physical activity may improve quality of life in patients with irritable bowel syndrome. Patients should be encouraged to increase their soluble fibre in their diet, for example, psyllium or ispaghula, as these improve bowel symptoms both in chronic constipation and in irritable bowel syndrome. Although patients treated with bran or psyllium may improve their constipation, approximately 60% of patients will report adverse events including abdominal pain. Patients with chronic abdominal pain may be treated with opiates and this will exacerbate their constipation further. It is essential to wean these patients off their opiates wherever possible.
Laxatives
The next step in the treatment algorithm is to prescribe an osmotic laxative. There are four main types of osmotic agents and these include polyethylene glycol-based solutions (Movicol), magnesium citrate-b ased products, sodium phosphate-b ased products, and non-absorbable carbohydrates. These products extract fluid into the intestinal lumen by osmosis and may occasionally cause diarrhoea. However, they are generally well tolerated. The magnesium hydroxide and other salts soften the stool and increase frequency of defecation. The absorption of magnesium is limited and is usually not a significant side effect (patients with renal impairment should be monitored closely). Sodium phosphate-based preparations should not be used long term as they can induce metabolic abnormalities.
Lactulose, which is used a lot in general practice, is associated with wind and abdominal pain and a Cochrane review suggested that polyethylene glycol laxatives were superior to lactulose in their effect and in their side effects.Stimulant laxatives such as bisacodyl and glycerine suppositories and sodium picosulphate and senna are widely used. However, they do cause some gut-related abdominal pain.
Newer agents such as lubiprostone and linaclotide act as secreta- gogues and increase intestinal chloride secretion by activating channels on the luminal side of the enterocyte. Water secretion follows the ion secretion and it is thought that the secretory affects are why these drugs accelerate small intestine and colonic transit.
Serotonin 5-HT4 receptor agonists induce mucosal secretion by activating submucosal neurons. The agonist most commonly used is prucalopride and this accelerates gastrointestinal and colonic transit in constipation. Side effects include abdominal pain and headaches in the first few days but these wear off rapidly. Much of the work for this drug was done in women and it is approved for use in women in whom laxatives failed to give adequate relief of symptoms.
Biofeedback
If laxative usage fails, patients should be treated with biofeedback- aided pelvic floor training. In patients with a hyposensitive rectum, sensory retraining can be added whereby a patient will learn to recognize weaker signals coming through and then attempt to defecate using abdominal and pelvic floor exercises. Up to two-thirds of patients with defecatory disorder have an improvement of symptoms with biofeedback but these treatments are time-consuming with patients required to attend hospital for five or six training sessions lasting 30-60 minutes each and the defecatory improvement may tail off without regular top-up sessions.
Surgery for constipation
Patients should only be referred for surgery after all non-surgical measures have failed and the symptoms continue to compromise daily life.
Constipation is associated with a poorer quality of life but has no mortality associated with it. However, surgery may cause considerable ongoing morbidity and potential mortality.Subtotal colectomy
Patients with isolated slow-transit constipation who have no evidence of pelvic floor dysfunction or diffuse gastrointestinal dysmotility are occasionally considered for a colectomy and ileorectal anastomosis. It is essential to advise these patients that the primary symptoms of constipation, for example, the infrequent and difficult evacuation, may be eliminated by this surgery, but other symptoms (particularly abdominal pain and bloating) will often persist postoperatively. During surgery, which is now done laparoscopically, the colon is removed to the level of the rectum. It is essential to preserve the presacral nerves and an ileorectal anastomosis should then be performed. Leaving any sigmoid colon or anastomosing the cecum to the rectum reduces the efficacy of this operation. This is not a procedure to be undertaken lightly as most series are associated with high morbidity and readmission rates. In a recent publication from the United States, the authors looked at the admissions for colectomies for constipation in two states from 1998 to 2011 (25). Over 400 patients had been operated during this time. There were no perioperative deaths in this series; however, perioperative complications occurred in 42.7% of the patients and a readmission rate of nearly 30% occurred within the first 30 days. As pointed out in this publication, constipation is a functional disorder that may have a significant impact on quality of life but no true morbidity or mortality. However, a significant number of patients in this series who had been operated on ended up with long-term complications.
Botulinum toxin for pelvic floor dysfunction
Patients who are seen to contract their puborectalis instead of relaxing it at the time of defecation may improve with biofeedback.
In the past, the puborectalis muscle has been divided and occasionally botulinum toxin has been injected into puborectalis muscle. The evidence for this is limited and this cannot be recommended at present for managing defecatory disorders.Stapled transanal resection
The stapled transanal resection (STARR) procedure was developed to try to correct two of the anatomical abnormalities that are seen on defecography associated with constipation. These are rectal intussusception, which is called occult rectal prolapse, and rectoceles (Figure 58.8a) The STARR procedure was introduced throughout Europe in the late 2000s and involved excising the redundant rectal mucosa associated with the rectocele and intussusception and reanastomosing using a staple line (Figure 58.8b). Placing a staple line within the rectum/pelvis has resulted in complications. Those reported in the literature include pain, urgency, and bleeding as well as more long-term infective complications such as pelvic sepsis, fistula, and bowel perforation. The long-term results of STARR are also not as good as were initially thought; it is presumed that the anatomical abnormalities that are corrected may actually be caused by the underlying disorder of function rather than causing the symptoms themselves. In general, there are fewer and fewer surgeons performing this procedure.
Lap ventral mesh rectopexy
As the knowledge and technical skills have improved, the procedure of a laparoscopic ventral mesh rectopexy, which was first proposed for external rectal prolapse by D'Hoore et al. (26) has been used more often for patients with rectal evacuatory disorders and rectal intussusception. The benefit of this procedure is an avoidance of posterior rectal mobilization, this preserves the autonomic nerves and hopefully reduces the postoperative complication of constipation seen with posterior rectopexy. The mesh is placed between the rectum and the vagina down to the pelvic floor and sutured onto the rectum and vagina closing the pouch of Douglas.
There is a relatively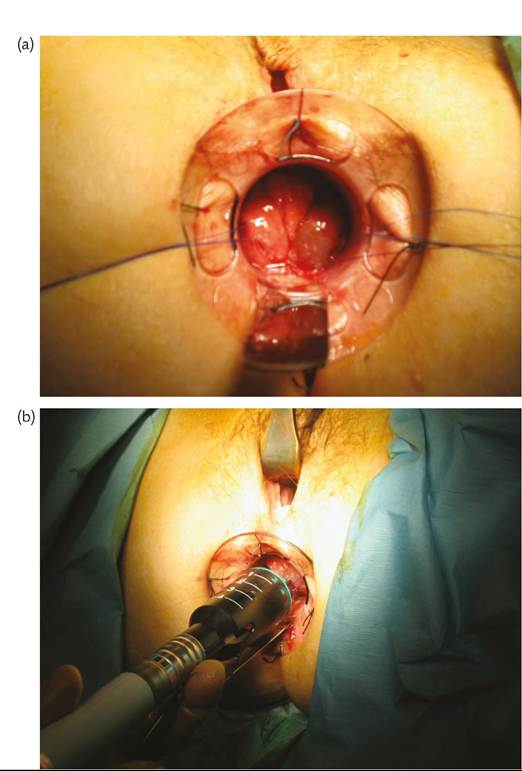
Figure 58.8 (a) Rectal intussusception. (b) STARR procedure resecting the rectal intussusception.
low morbidity rate of 8-10% with this procedure but there are concerns about mesh-related complications which may occur in at least 4.6% of patients (27).
Many of the published studies include patients with full-thickness rectal prolapse and those with internal intussusception and obstructive defecation. A recent study of 100 women with internal rectal prolapse treated with a laparoscopic ventral mesh rectopexy (using a biological mesh) found that constipation was cured in 79% and improved in 92%. Many patients with intussusception suffer from incontinence as well as difficulty in evacuation and the incontinence was improved in 86% of patients (28).
Concerns continue with regard to the potential for mesh erosions using this procedure. A multicentre collaboration looked at 2203 patients undergoing this type of surgery in the United Kingdom. It was a retrospective study, with short and minimal follow-up. Forty-five patients (2%) are known to have had erosions and this almost certainly is an underestimate. Eighteen patients had major morbidity associated with the erosion and the mesh removal (29).
This procedure has potential to help treat patients with intussusception and complex evacuatory disorders but patients should be
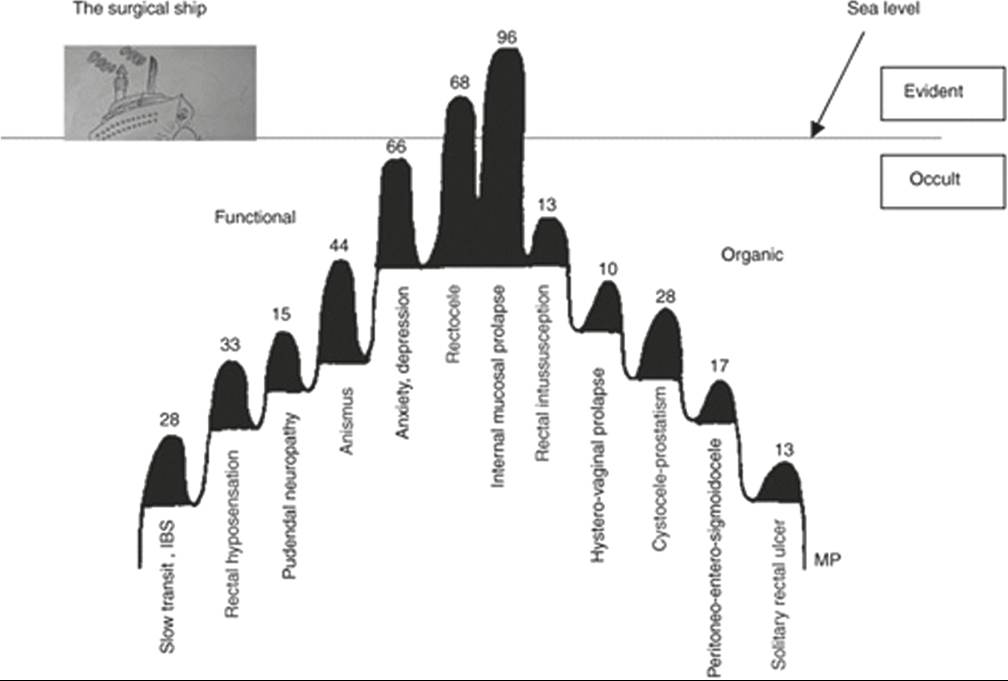
Figure 58.9 There are many other issues in patients presenting with constipation.
carefully counselled as to the potential for complications and major morbidity if the mesh erodes (Montgomery v Lanarkshire Health Board (2015)-a legal ruling).
Summary
The symptoms of constipation occur in a large percentage of the general population. The impact on quality of life when they occur for a long period of time is large. However, patients often have many coexisting other pelvic floor disorders. Pescatori et al. coined the term ‘iceberg effect’ to explain that while presenting with one symptom or anatomical issue, most patients will have a collection of other problems (30) (Figure 58.9).
This study looked at a series of 100 consecutive constipated patients. Although it found that 54% patients had both a rectocele and mucosal prolapse, all 100 patients had at least two further obstructive defecation-related problems. The commonest three issues were anxiety-depression, anismus, and rectal hyposensation (66%, 44%, and 33% respectively). The median number of occult disorders was five (range two to eight). The majority of patients were treated conservatively and only 14% required surgery.
Although there are surgical options available, it is important to treat conservatively and understand the complexity of the other issues involved in patients presenting with constipation.