Infective Endocarditis
The diagnosis of infective endocarditis is based on clinical, echocardiographic, and bacterial culture data. HIV-infected patients usually present with fever, sweats, weight loss, coexisting pneumonia, and/or meningitis.
Among intravenous drug addicts, the tricuspid valve is most frequently affected (Fig. 1). Vegetations may form on the tricuspid or pulmonic valves with resultant pulmonary embolism and consequent septic pulmonary infarcts that appear as multiple opacities on chest radiograms. Systemic emboli may involve the coronary arteries, spleen, bowel, extremities, and central nervous system. Cardiac rhythm alterations (i.e., atrioventricular block) may suggest the presence of an abscess in proximity to the atrioventricular node. Peripheral pulses must be examined for signs of embolic occlusion or pulsating mass suggesting mycotic aneurysm. Mycotic aneurysms may occur in the intracranial arteries potentially leading to intracranial hemorrhage.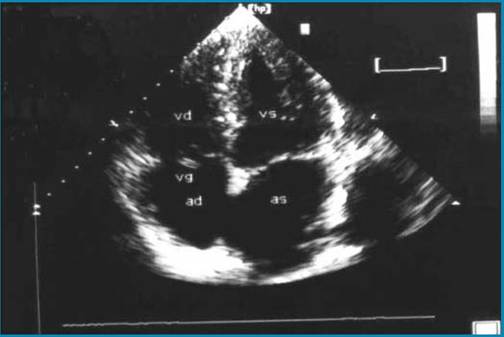
Fig. 1. Echocardiographic finding of Candida endocarditis in an intravenous heroin user suffering from AIDS. A vegetation (vg) is attached to the anterior leaflet of the tricuspid valve (apical four-chamber view). ad, right atrium; as, left atrium; vd, right ventricle; vs, left ventricle. (From [1], with permission from Elsevier)
Echocardiographic findings in endocarditis include mobile echodense masses attached to the inflow side of the valvular leaflets or mural endocardium; pericardial effusion is frequently associated with this. Transthoracic echocardiography (TTE) is useful for detecting relatively large valvular mass(es); however, perivalvular abscess, leaflet perforation, or rupture of the valvular chordae are better assessed by transesophageal echocardiography (TEE).
Both TTE and TEE, which may be performed in the ED, are also useful in guiding the duration of antibiotic therapy and evaluating the timing for surgery when necessary.Assessment of infective endocarditis in an HIV-infected patient should include at least four sets of blood cultures separated by 30 min. Empiric broad-spectrum antibiotic therapy should be started within a maximum of 2-3 h from admission of the patient to the ED (after blood culture sets are obtained). According to our clinical experience, combination regimens including vancomycin 15 mg/kg i.v. (maximum 1 g) every 12 h, ampicillin 2 g i.v. every 4 h, and gentamycin 1 mg/kg i.m. every 8 h have significant bactericidal activity and cover methicillin-resistant Staphylococcus aureus [1].
Nonbacterial thrombotic endocarditis, also known as marantic endocarditis, is most common in patients with HIV wasting syndrome [1]. The incidence of marantic endocarditis and systemic embolization from marantic endocarditis is a rare cause of death in AIDS patients receiving HAART, whereas its frequency is increasing in developing countries (about 10%), where HAART availability is scanty, with a high mortality rate for systemic embolization [5].