Pericardial Effusion
Pericardial effusion in HIV disease is generally related to opportunistic infections (Mycobacterium tuberculosis, M. avium intra- cellulare, S. aureus, Nocardia asteroides, Rhodococcus equi, Listeria monocytogenes, Chlamydia trachomatis, coxsackievirus, Epstein-Barr virus, cytomegalovirus, adenovirus, herpes virus, Histoplasma capsula- tum, Cryptococcus neoformans, and Toxoplasma gondii), or to malignancy (Kaposi’s sarcoma, non-Hodgkin’s lymphoma), but most often a clear etiology is not found.
Fever, chest pain radiating to the left shoulder (often dull), aggravated by a supine posture and often decreased by sitting up and leaning forward, and pericardial friction rub (over the left sternal border, usually accentuated by sitting up and leaning forward) should suggest acute pericarditis. Pericardial effusion is suggested by absence or weakness of the apical impulse with an apparent increase in the area of dullness to percussion over the left chest and over the hepatocardiac angle as well as by muffled heart sounds, diffuse low-voltage ECG, electrical alternans of QRS complexes, and increased cardiac opacity on chest radiographs. Echocardiography confirms clinical suspicion by showing the pericardial effusion (Fig. 2a-b). An M-mode technique may help to demonstrate characteristic signs of cardiac tamponade: right atrial compression and diastolic right ventricular collapse. These echocardiographic signs pre-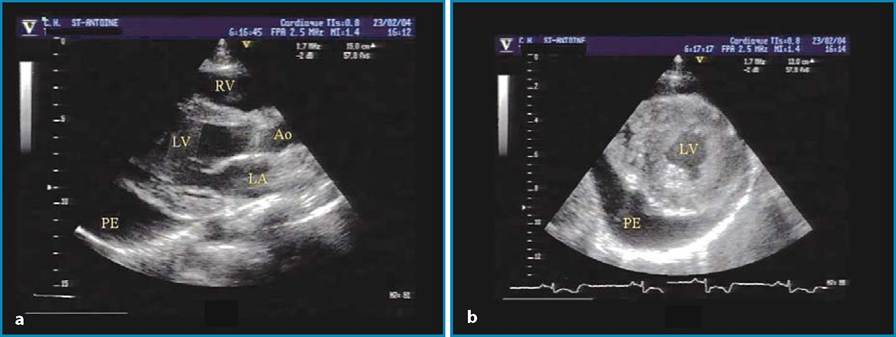
Fig. 2a, b Echocardiographic finding of posterior pericardial effusion in an AIDS patient. a Parasternal long-axis view; b Parasternal short-axis view; LV, left ventricle; RV, right ventricle; Ao, aorta; LA, left atrium; PE, pericardial effusion
cede pulsus paradox or severe dyspnea related to the hemodynamic effects of cardiac tamponade. CT scans can easily demonstrate pericardial effusion and help analyze the thickness of the pericardium and reveal signs of constrictive pericarditis (Fig. 3).
Pericardial effusion may resolve spontaneously in up to 42% of HIV-positive patients [1]. Pericardiocentesis is currently recommended only in large or poorly tolerated effusions, for diagnostic evaluation of systemic illness, or in the presence of cardiac tamponade [1].