Introduction
Highly active antiretroviral therapy (HAART) has decreased by two-thirds [1] the lethality of AIDS and opportunistic infections. However, the improved survival of HIV patients receiving HAART has become associated with metabolic complications including insulin resistance, impaired glucose tolerance, loss of skeletal muscle mass (sarcopenia) and performance, osteopenia, lipid abnormalities such as dyslipidemia and body-fat distribution [2-19], which increase cardiovascular morbidity, compromising the patient’s quality of life and the efficacy of HAART.
As a consequence of prolonged survival and the direct effect of HAART [16], AIDS is changing from a “slim disease” to a “lipodystrophic disease” [20] and the care of the HIV-infected patients “has shifted from prevention and treatment of opportunistic infections and malignancies to management of the metabolic and related complications’ll?]. The risk of cardiovascular disease (CVD) in HIV patients is increased two- to three-fold by disturbances in fat metabolism [15, 17]. New strategies addressed to prevent and manage such emerging disorders, including muscle and bone disorders (sarcopenia and osteopenia) [17, 21, 22], are needed. Moreover, coronary heart disease (CHD) is the leading cause of death and a common cause of morbidity in Western countries. Approximately 14 million Americans have CHD, according to NHANES III data [23]. Annually, about 1.1 million of them experience a heart attack and about 500,000 die from CHD (Fig. 1).The objective proposed by various health authorities for the year 2010 is to reduce CHD deaths to no more than 51 in 100,000, “enhancing the cardiovascular health and quality of life of all Americans through improvement of medical management, prevention and control of risk factors, and promotion of healthy lifestyle behaviors” [24]. In light of this policy also adopted by the European Union, particular attention must be devoted to HIV-infected individuals who, in the near future, could represent an emerging population at a more elevated risk of CHD due to the prolonged life expectancy and/or metabolic disturbances induced by therapy [25-30]. Elevated triglycerides (TG), low-density lipoprotein (LDL) cholesterol, very low-density lipoprotein (VLDL) cholesterol, and reduced levels of high-density lipoprotein (HDL) cholesterol are associated with body-fat redistribution characterized by visceral fat accumulation, peripheral lipody- strophy/lipoatrophy, and CHD.
It has been reported that 5-75% of HIV patients receiving HAART experience a worse lipid metabolism and body-fat distribution after 10-12 months of therapy [15, 17].Our guidelines, based on our own and the experience of others [31-37], meet the intervention criteria defined by the American National Cholesterol Education Program (NCEP) [38], including evaluation criteria, diet prescription, drug and exercise treatment — preliminary discussion included in The Pavia Consensus Statement, Octo-
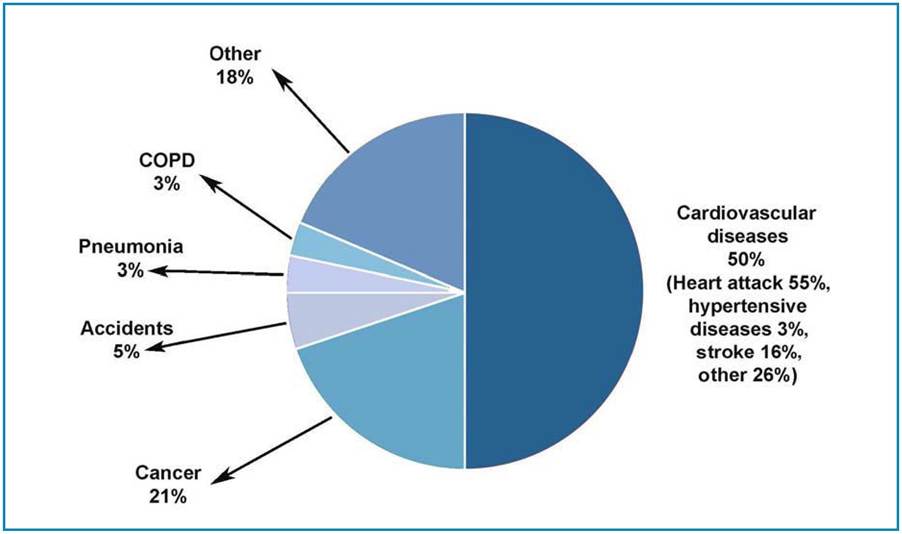
Fig. 1 Cardiovascular diseases account for 50% of the total deaths in the United States. COPD, chronic obstructive pulmonary disease
ber 2001 [39, 40], the recommendations of the HIV Medicine Association of the Infectious Disease Society of America and the Adult AIDS Clinical Trials Group (AACTG) [41], and the 2007 updated scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity and Metabolism [42]. Our study is also based on algorithms and approaches developed in classic physiology and sports Medicine for healthy people, the elderly, diseases such as diabetes and CVD [42-48].