Investigations
Symptoms of cough and dyspnoea with or without fever and sweats identify the presence of respiratory disease in HIV positive patients, but these are non-specific and symptomatic patients should be investigated.
Non-invasive investigations
These tests should ideally allow a specific diagnosis to be made and a therapeutic response monitored by a quick, cheap and universally available method.
Unfortunately, none of these tests fulfils the criteria but they do help to:• Determine the presence or absence of pulmonary disease.
• Assess disease severity.
• Determine if an invasive test is indicted to make an aetiological diagnosis.
Box 6.2 Investigation of respiratory disease
Non-invasive tests
Chest radiograph
Arterial blood gases or oximetry
Pulmonary function tests
Invasive tests
Induced sputum
Fibreoptic bronchoscopy and bronchoalveolar lavage with or without transbronchial biopsy
Open lung biopsy
Chest radiology
The chest radiograph may be normal in HIV positive patients with respiratory disease caused by P. carinii pneumonia. The most common abnormality seen in patients with pneumocystis pneumonia is bilateral perihilar haze which may be very subtle and easy to miss. More severely unwell patients may have more diffuse interstitial shadowing which may progress to severe consolidation with “white out” throughout both lung fields, with sparing of the apices and costophrenic angles. These radiographic appearances are non-specific and may also be seen in pyogenic bacterial, mycobacterial and fungal infection, and also in Kaposi’s sarcoma and lymphoid interstitial pneumonitis. Between 5% and 10% of patients with pneumocystis pneumonia have atypical chest radiographs showing cystic changes, upper lobe infiltrates mimicking tuberculosis, hilar or mediastinal lymphadenopathy or focal consolidation.
The chest radiograph in pneumocystis pneumonia may deteriorate very rapidly from being normal to showing severe abnormality in just a few days. By contrast, radiographic recovery can be slow. Nodular shadowing, adenopathy and pleural effusions on the chest radiograph suggest Mycobacterium tuberculosis, Kaposi’s sarcoma or lymphoma.
Figure 6.1 Chest radiograph of patient with early pneumocystis pneumonia
Arterial blood gases and oximetry
Hypoxaemia and a widened alveola-arterial oxygen gradient are very sensitive for the diagnosis of pneumocystis pneumonia but may also occur in other conditions. Exercise-induced arterial desaturation detected by oximetry is also sensitive for the diagnosis of pneumocystis pneumonia; desaturation may persist for several months following recovery from P. carinii pneumonia and occur also rarely in cytomegalovirus pneumonitis but is unusual in other respiratory conditions.
Pulmonary function tests
The single breath carbon monoxide transfer factor (TLCO), transfer coefficient (KCO), total lung capacity (TLC) and vital capacity (VC) may all be reduced in patients with pneumocystis pneumonia. Reductions in TLCO to 70% of predicted normal occur in HIV positive patients with pneumocystis and other respiratory disease, including Kaposi's sarcoma and bacterial infections, so this finding is not specific.
Invasive tests
These allow an aetiological diagnosis to be made.
Sputum induced by hypertonic saline
This procedure must be carried out away from other patients and staff in a separate room, ideally with “negative pressure” facilities in order to reduce the risk of nosocomial transmission of infection including tuberculosis. The patient inhales 20-30 ml of 2.7% (3N) saline through an ultrasonic nebuliser. Saline deposits in the peripheral airways and alveoli, causing irritation and inducing bronchial secretion. Fluid is also drawn into the airways from the interstitium, loosening inflammatory exudate and casts from alveoli.
These are mobilised by the mucociliary escalator and move centrally where they are coughed out by the patient. Careful preparation of the patient is needed, including starving for several hours before the procedure and rigorous cleansing of the mouth to remove oral debris so that the sputum sample is not contaminated (food debris and squames take up stain and make analysis difficult). Purulent samples of sputum suggest a bacterial cause. P. carinii infection is usually found in clear “saliva-like” samples that become viscid on cooling to room temperature. Fungal infection and mycobacterial infection may also be diagnosed by this technique. Many centres do not carry out sputum induction because of the need for special equipment and the low yield when the technique is compared with fibreoptic bronchoscopy, both for the diagnosis of pneumocystis pneumonia and other pathogens. Some patients find sputum induction unpleasant and become nauseated or dyspnoeic. Arterial desaturation may also occur during the procedure.Fibreoptic bronchoscopy
Bronchoscopy allows inspection of the bronchi to be carried out and lesions of Kaposi's sarcoma may be identified.
Bronchoalveolar lavage is routinely carried out from the middle lobe or from the area of maximum abnormality seen on the chest radiograph. Transbronchial biopsies are now rarely done as they add little to the diagnostic yield for P. carinii and other diagnoses, and the technique is associated with adverse effects including haemorrhage and pneumothorax. If transbronchial biopsy is not performed a diagnosis of non-specific or lymphocytic interstitial pneumonitis might be missed.
Open lung biopsy
It is rarely necessary to carry out open lung biopsy because of the high yield from bronchoalveolar lavage. This investigation may be necessary if fibreoptic bronchoscopy and lavage fail to

Figure 6.2 Chest radiograph of patient with severe pneumocystis pneumonia
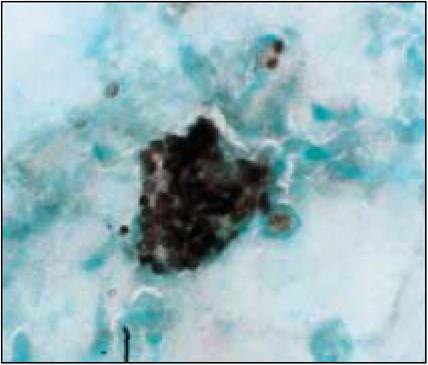
Figure 6.3 Cytology preparation of induced sputum showing many cysts of Pneumocystis carinii (Grocott's methenamine silver stain)
Box 6.3 Open lung biopsy
If fibreoptic bronchoscopy and lavage fail to identify diagnosis
or
where patient with bronchoscopic diagnosis deteriorates despite specific treatment
identify a diagnosis or in cases where a patient with a bronchoscopic diagnosis, deteriorates despite specific treatment.
The presenting clinical features and treatment of the common pulmonary manifestations of HIV disease are described below.