Pneumocystis carinii pneumonia
Despite widespread use of anti-pneumocystis prophy!axis and HAART, P carinii pneumonia remains a common AIDS-defining diagnosis in patients who at presentation with pneumonia are unaware of their HIV serostatus or who, despite knowing they have HIV infection, are non-compliant with or intolerant of their prophylaxis and/or HAART.
Patients complain of a non-productive cough and increasing dyspnoea (over two to three weeks or more); they may also have fever and sweats. The chest radiograph may be normal or show interstitial infiltrates: in severe pneumonia there may be widespread alveolar consolidation.
Treatment
It is important to assess the severity of the pneumonia in order to choose appropriate treatment, as some drugs are ineffective in severe disease. High-dose co-trimoxazole remains the “gold standard” treatment. Treatment is for 21 days, given intravenously for the first 10—14 days, diluted in 1 in 25 of 0.9% saline, subsequently, orally. Patients with mild disease may be treated with oral co-trimoxazole from the outset. The principal side-effects are nausea and vomiting, leucopenia and rash. Routine use of folic or folinic acid does not prevent leucopenia and may be associated with increased therapeutic failure. HAART is usually stopped while co-trimoxazole is being given to avoid profound myelosuppression. Conventionally used doses of co-trimoxazole (20 mg/kg day of the trimethoprim component) may be excessive: dose reduction to 75% of this dose (to maintain serum trimethoprim concentrations at 5—8 μg∕ml) has equivalent efficacy and reduced toxicity.
Alternative treatment regimens include:
Clindamycin-primaquine combination (clindamycin 600 mg ?4∕day iv or orally and primaquine 15 mg/day orally) has been used in patients intolerant of, or failing to respond to, co-trimoxazole. Principal side-effects are rash, nausea and vomiting, and leuco(neutro)penia.
Dapsone-trimethoprim (100 mg/day dapsone and 20 mg/kg/day trimethoprim) given orally for 21 days is as effective as oral co-trimoxazole in mild to moderate disease and is better tolerated by patients. Side-effects include methaemoglobinaemia and hyperkalaemia, nausea and rash.
Atovaquone suspension (750 mg ? 2∕day) given orally for 21 days is less effective (and less toxic) than either co-trimoxazole or pentamidine for mild to moderate disease. Absorption from the gut is variable but may be increased if taken with food.
Pentamidine is not often used because of significant toxicity and because other regimens have similar efficacy and less toxicity. It is given at a dose of 4 mg/kg/day (of the isethionate salt) given diluted in 250 mg 5% dextrose by slow intravenous infusion (over 2 hours); it should not be given by intramuscular injection. The major side-effects are hypotension and hypoglycaemia; nephrotoxicity with increases in creatinine and urea concentrations may occur. Dose reduction to 3 mg/kg/day is associated with reduced toxicity but may be less effective. Blood pressure and blood glucose concentrations should be closely monitored. Response to pentamidine (defervescence of fever, reduction in dyspnoea and improvement in blood gases) may take longer (4—7 days) than intravenous co-trimoxazole.
Table 6.1 Grading of severity of P, carinii pneumonia
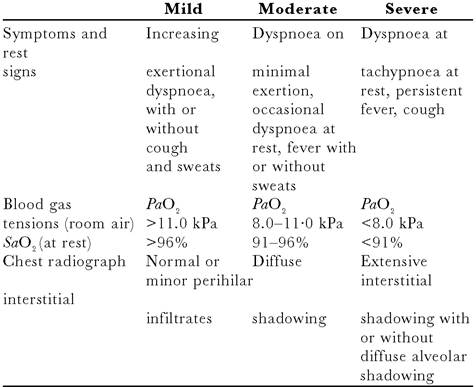
PaO2 = partial pressure of oxygen; SaO2 = arterial oxygen saturation, measured with a transcutaneous pulse oximeter.
Table 6.2 Treatment of P. carinii pneumonia
id="Picutre 49" class="lazyload" data-src="/files/uch_group75/uch_pgroup303/uch_uch7201/image/image049.jpg">
coids
Box 6.4 Adjuvant glucocorticoids in moderate/severe pneumonia
• Reduce risk of respiratory failure (by 50%)
• Reduce risk of death (by 33%)
• Should be started at same time as specific anti-pneumocystis treatment
Nebulised pentamidine is now no longer used to treat P.
carinii pneumonia as there are several other more effective therapies and because this form of treatment does not suppress the development of extrapulmonary pneumocystosis.Adjuvant glucocorticoids for patients with moderate or severe pneumocystis pneumonia reduces the risk of respiratory failure (by up to 50%) and the risk of death (by up to 33%). Glucocorticoids should be started together with specific anti- pneumocystis treatment in any patient presenting with a PaO2 of 9.3kPa breathing air. In some patients this will be on the basis of a presumptive diagnosis; clearly there will be a need to confirm the diagnosis rapidly. Treatment is with intravenous methylprednisolone 1 g/day for three days, followed by 0.5g for two days, followed by oral prednisolone 40 mg daily tailing off over 10 days. Alternatively, prednisolone 40 mg orally twice daily is given for 5 days and then gradually reduced over 21 days (or intravenous methylprednisolone is given at 75% of these doses).
Intensive care
Over 90% of patients respond to treatment and survive their first episode of pneumocystis pneumonia. In those who fail to respond and who develop respiratory failure, mortality is 50%. Transfer to the intensive care unit for mask CPAP ventilation or intubation and mechanical ventilation should be considered in this situation. When considering the appropriateness of intensive care, assess the patient's wishes and those of their partner and relatives as well as the patient's previous and expected quality of life in relation to their HIV disease.
Prophylaxis
HIV positive patients, including those receiving HAART should receive primary prophylaxis against P. carinii pneumonia if they have a CD4 count < 200 cells∕μl or a history of oral/pharyngeal candidiasis or if they have a CD4 lymphocyte count 10 000 units∕m2 and vincristine 2 mg once every three weeks. Liposomal formulations of daunorubicin and doxorubicin may also be used as single-agent chemotherapy.
Treatment of pleural effusions (which occur secondary to Kaposi's sarcoma on the visceral pleura or to mediastinal glands) is problematical. Chemical pleuradesis is rarely successful and radiotherapy has not been shown to be of value.Box 6.6 Bacterial infections
• Increased incidence of sinusitis, bronchitis and pneumonia in HIV infected persons, compared to general population
• Bacterial infection especially common in HIV infected IVDU
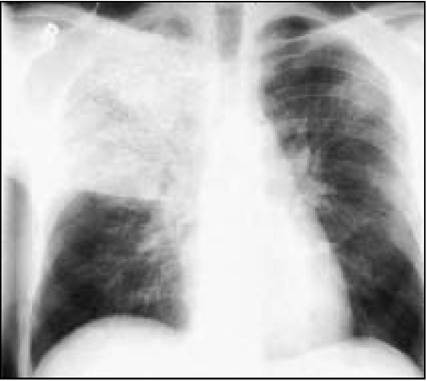
Figure 6.6 Chest radiograph showing lobar pneumonia due to Streptococcus pneumoniae

Figure 6.7 Chest radiograph of pulmonary Kaposi’s sarcoma showing multiple pulonary nodules
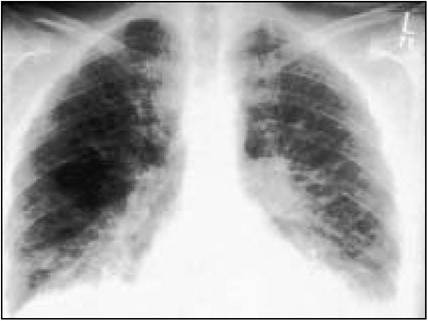
Figure 6.8 Chest radiograph of pulmonary Kaposi’s sarcoma showing bilateral pleural effusions and interstitial infiltrates
More on the topic Pneumocystis carinii pneumonia:
- Pneumocystis carinii pneumonia
- Protozoal infections
- Pneumocystis carinii and Pneumocystis wakefieldiae Infections: Pneumocystosis
- Box 1.1 Early history of the epidemic
- Pneumocystis murina Infection: Pneumocystosis
- PNEUMOCYSTIS INFECTIONS
- Natural history and clinical manifestations
- Aspiration Pneumonia
- Investigations
- The lungs are commonly affected in patients infected with HIV, with over 60% of patients having at least one respiratory episode during the course of their disease.