Pneumocystis carinii and Pneumocystis wakefieldiae Infections: Pneumocystosis
Laboratory rats have been central to understanding the biology of Pneumocystis. Rats were recognized to develop pneumonias caused by a new organism that had features similar to human disease.
Although not the first host species to be shown to be infected with Pneumocystis (guinea pigs get that honor), rats were definitively shown to be infected with a similar agent that was the first Pneumocystis to be named: Pneumocystis carinii. Because the organism cannot be cultured or propagated in vitro, the rat became an important model and source of infectious organisms, which has given way to immunodeficient mice in recent years. For many years, Pneumocystis was thought to be a protozoan, giving way to terminology that continues in use today, including trophozoites, cysts, and sporozoites. It became apparent in early studies that there was a high degree of host species specificity among Pneumocystis organisms. The advent of molecular sequencing revealed the true complexity of this genus, finally recognizing Pneumocystis to be a fungus, and giving rise to a multitude of new names and species. Human pneumocystosis is now recognized to be caused by human-specific Pneumocystis jiroveci, but physicians continue to use "PCP” (P. carinii pneumonia) as a common term for the human condition. Since P. carinii was initially assigned to the rat, rats have been awarded this species as their own. It is now recognized that rats can serve as hosts to at least 5 species of Pneumocystis, and laboratory rats have been shown to be host to 2 of those species, including P. carinii and P. wakefieldiae. The former is the most common among laboratory rats, but dual infections occur. The mouse agent is genetically distinct, and named Pneumocystis murina.Pulmonary lesions associated with Pneumocystis infection and propagation of organisms have been produced in young laboratory rats from infected colonies that were treated for several weeks with immunosuppressants such as cortisone and fed a protein-deficient diet.
Steroid-treated female rats develop the disease at a faster rate than male rats. Spontaneous pneumocystosis has been recognized in athymic rats. During the late 1990s, inflammatory lesions were noted in young immunocompetent rats, which were attributed to a putative viral agent called "rat respiratory virus (RRV).” Recent studies have revealed that RRV is Pneumocystis, rather than a virus. Pneumocystis is transmitted by aerosol exposure during the neonatal period. Six- to twelve- week-old rats are optimal shedders of Pneumocystis, after which time Pneumocystis numbers decline until they are completely cleared from the immunocompetent host. Infection within an enzootically infected population is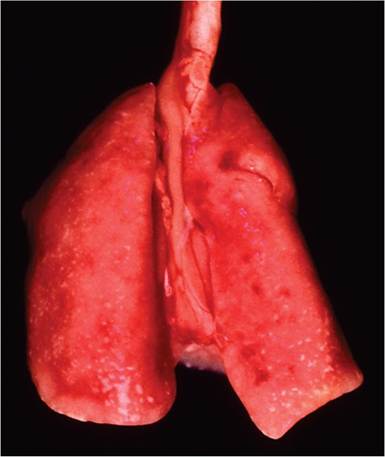
FIG. 2.45. Lungs from an immunocompromised rat with pneumocystosis. Note the failure to collapse and the raised foci in the subpleural regions consistent with focal cellular infiltrates.
maintained by spore-shedding young rats that transmit infection to 3-4-week-old weanling rats with declining maternal antibody.
Pathology
In severely affected animals, clinical signs include dyspnea, cyanosis, and weight loss. There is diffuse to focal consolidation, lungs collapse poorly, and frequently, they have an opaque pale pink color (Fig. 2.45). On microscopic examination, there is alveolar flooding with foamy, eosinophilic material, presenting a honeycomb appearance (Fig. 2.46). In athymic rats, pulmonary lesions vary from mild interstitial pneumonia with
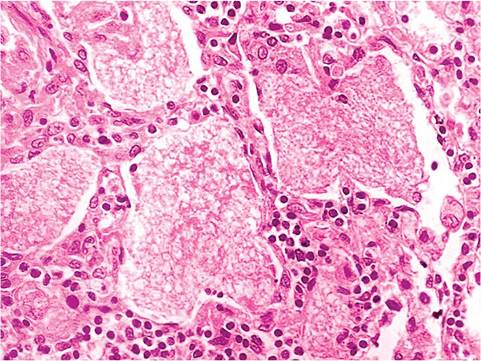
FIG. 2.46. Lung from a rat with pneumocytosis. Alveoli are flooded with foamy material containing Pneumocystis organisms and the interstitium is infiltrated with mononuclear leukocytes.
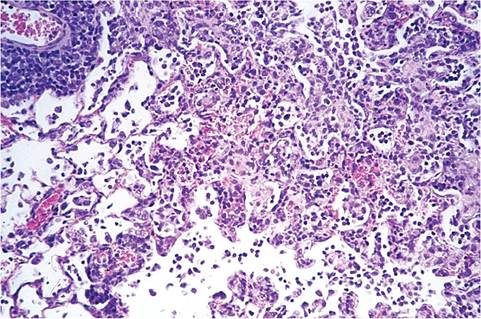
FIG. 2.47. Lung from a young rat with pulmonary lesions that were once attributed to “rat respiratory virus” infection, but have been found to be due to Pneumocystis sp.
infection. Note the perivascular lymphocytic infiltrates, interstitial pneumonia, and the marked alveolar histiocytosis.scattered alveolar macrophages to severe interstitial pneumonia with the alveoli distended with typical foamy material. In more advanced cases, in addition to the infiltrating inflammatory cells and the foamy alveolar exudate, there is marked proliferation of type II pneumocytes and interstitial fibrosis. In sections stained using procedures such as the Grocott modification of Gomori's methenamine silver technique, numerous black trophozoites and yeast-like cysts 3-5 μm in diameter are present singly or in groups within alveoli. Ultrastructural examination reveals trophozoites with filapodia in close association with type I pneumocytes.
Conventionally housed, young immunocompetent rats may develop transient multifocal nonsuppurative perivasculitis and interstitial pneumonia (Fig. 2.47), which may persist for several weeks. A scattering of neutrophils and focal hyperplasia of type II pneumo- cytes have also been observed during the course of the infection. Airways are usually spared, although there may be lymphocytic infiltrates around some bronchioles. These lesions were once considered to be due to RRV, but are now known to be associated with Pneumocystis infection. In the absence of an immunodeficient state (e.g., athymic rats), these lesions are far more likely to be encountered than the classic lesions of pulmonary pneumocystosis.
Diagnosis
The distinctive pulmonary lesions and the demonstration of the cyst forms (see Mouse Chapter 1, “Pneumocystis murina Infection”) during active infection, using silver-staining procedures on impression smears of lung or in paraffin-embedded specimens, is generally used to confirm the diagnosis. PCR can be used to detect the organism in specimens collected from lung tissue, by bronchioalveolar lavage, or with oral swabs.
More on the topic Pneumocystis carinii and Pneumocystis wakefieldiae Infections: Pneumocystosis:
- Pneumocystis carinii and Pneumocystis wakefieldiae Infections: Pneumocystosis
- PNEUMOCYSTIS INFECTIONS
- BIBLIOGRAPHY FOR BACTERIAL AND FUNGAL INFECTIONS