Pneumocystis murina Infection: Pneumocystosis
Pulmonary pneumocystosis is a common finding in immunodeficient strains of mice, and may be a lifelimiting disease in these strains. It may also occur to a lesser degree in aging immunocompetent mice.
Although it was once thought that pneumocystosis in the mouse was due to Pneumocystis carinii, it is now known that there are many host-specific Pneumocystis species. Pneumocystosis in the mouse is due to infection with mouse-specific P. murina.Epizootiology and Pathogenesis
Nonfilamentous yeast-like trophic forms adhere to type I pneumocytes with clusters of developmental stages extending into the alveolar lumen. These forms have abundant thin filopodia. Asci (cysts) are also present, and contain eight ascospores. Pneumocystis murina isolated from laboratory and wild mice are genetically similar. Normally, infection is subclinical and probably transient in immunocompetent mice. Immunosuppression of subclinically infected mice may result in development of Pneumocystis pneumonia and more efficient transmission to contact animals. Spontaneous enzootics of Pneumocystis pneumonia are now common in a variety of immunodeficient strains of mice. Superimposed viral infection can exacerbate disease, and superimposed bacterial infections, such as Pasteurella pneumotropica, may result in suppurative bronchopneumonia. Immunocompromised mice subclinically infected with P. murina inoculated with PVM developed severe respiratory tract lesions attributed to the dual infection.
Pathology
Clinical signs of pneumocystosis in immunodeficient mice include dyspnea, wasting, hunched posture, and dry, scaly skin. Lungs collapse poorly and have a rubbery consistency, with pale, patchy areas of consolidation (Fig. 1.82). Microscopic examination reveals interstitial pneumonitis, with proteinaceous exudation into the alveolar lumina. There is marked thickening of alveolar septa and infiltration with mononuclear leukocytes (Fig.
1.83). Finely vacuolated, eosinophilic material containing punctate cyst forms and alveolar macrophages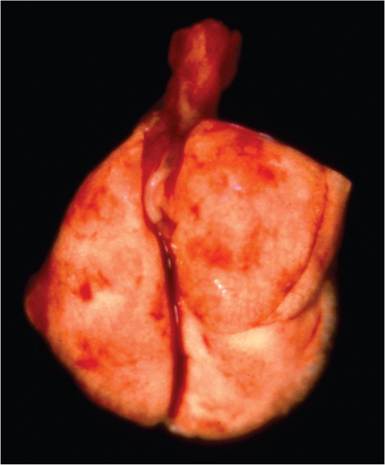
FIG. 1.82. Lungs from an immunodeficient mouse with Pneumocystis murina pneumonia. The lungs are pale, fleshy, and collapse poorly, typical gross findings with this disease.
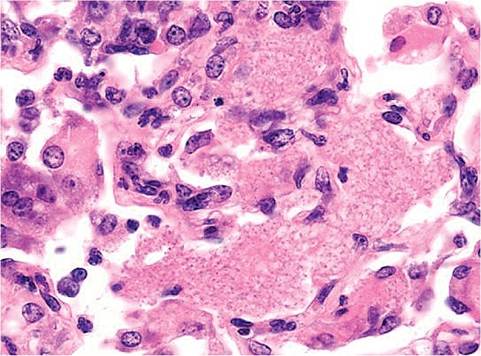
FIG. 1.83. Lung from an athymic mouse with spontaneous Pneumocystis murina pneumonia. Alveolar septa are hypercellular, with mononuclear cell infiltration. Foamy proteinaceous exudate containing punctate P. murina cyst forms is present in alveoli.
are scattered in affected alveoli. In tissue sections stained with the PAS or methenamine silver procedures, numerous rounded and irregularly shaped 3-5 μm cyst forms are present in affected areas (Fig. 1.84). Electron microscopy reveals numerous trophic forms with long filapodia intermixed with thicker walled asci. The quality of the pneumonia associated with Pneumocystis in immunodeficient mice can be quite variable, depending upon the immune deficiency. Some types of mice may have very few visible cysts or alveolar exudation, with principally an interstitial pneumonia. Extrapulmonary infection of other tissues, including bone marrow, heart, liver, and spleen, may be encountered in SCID mice. Aged immunocompetent mice may develop focal areas of alveolar pneumocystosis as an incidental finding.
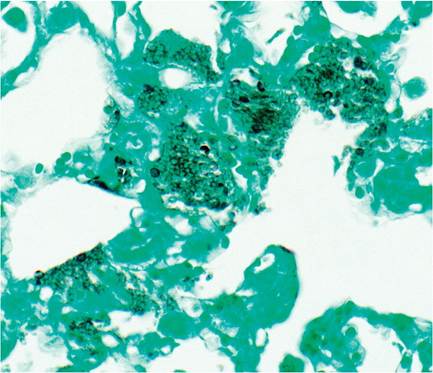
FIG. 1.84. Lung from a mouse with Pneumocystis murina pneumonia. Large numbers of cyst forms are present in alveoli (methenamine silver stain).
Diagnosis
A history of experimental procedures leading to immunosuppression or disease in genetically immunodeficient mice is a critical predisposing factor. Organisms may be demonstrated in the typical foamy alveolar exudate, using methenamine silver or PAS stains. Differential diagnoses for chronic progressive pneumonia in immunodeficient mice include viral pneumonitis due to Sendai virus and PVM and pulmonary edema secondary to congestive heart failure. Coinfections with respiratory viruses or Pasteurella pneumotropica are known to aggravate pulmonary pneumocystosis. PCR can be used to screen for P. murina infection, but it is important to test young mice, as infection is transient in immunocompetent animals.